Download
1 / 67
680 likes | 887 Views
Improving the Quality of Stroke Care. Tony Rudd. “it is the duty of the physician to explain to the patient, or to his friends, that the condition is past relief, that medicines and electricity will do no good, and that there is no possible hope of cure” William Osler. St Thomas’ Hospital.

E N D
Improving the Quality of Stroke Care Tony Rudd
“it is the duty of the physician to explain to the patient, or to his friends, that the condition is past relief, that medicines and electricity will do no good, and that there is no possible hope of cure” William Osler
St Thomas’ Hospital Stroke Care in 1988 • Patients admitted under care of any of 17 general physicians to any one of 15 wards • Very little happened acutely • Brain scans difficult to obtain and therefore rarely done • Referred to geriatricians for rehabilitation – long wait • No stroke specialist service either in hospital or community
The EC BIOMED 1 & 2 Stroke Project (Adjusted incremental costs (US$/PPP) and hazard ratios (with 95% CI) by centre (Riga (Latvia) as reference) The EC BIOMED 1 Stroke Project) Grieve R et al. Stroke 2001
What are the problems that still need solving? • Unacceptable variation in the quality of care between hospitals • Variable quality of clinical and managerial leadership • Variable resources provided for stroke care • UK slow to adopt new technologies e.g. Thrombolysis • Still a belief amongst many people (professionals and public) that stroke untreatable disease of old people
Early Stroke Audit Results (1998/9) • 18% of patients through stroke unit • 23% cognitive assessment • 44% visual fields recorded • 55% rehabilitation goals set • 41% G.P. contacted within 3 days of discharge
Key Forces for Change • Research • Guidelines summarising the research evidence and clinical consensus (RCP Guidelines and NICE Guidelines on Acute Stroke and TIA and NICE Technology Appraisal on alteplase) • National Audit • Sentinel audit • SINAP • Carotid endarterectomy audit • National Audit Office report • National Stroke Strategy
Key Forces for Change • NICE Quality Standards • Commissioning Outcomes Framework (COF) standards • Performance standards set by Care Quality Commission • Stroke Improvement Programme and Stroke and Cardiac Networks • Stroke Research Network • Public opinion • Media reports • Voluntary sector campaigning
Stroke Programme at the RCP • Guidelines • NICE Guidelines on Acute care and TIA • Intercollegiate Guidelines on the rest • 4th edition to be published Sept 2012 • National Audit • Sentinel audit (1998-2012) • Carotid interventions audit • Acute Continuous Stroke Audit (SINAP) • SSNAP • Change management • Presentations • Workshops • Peer Review • Politics/lobbying • Stroke Improvement Programme links
History of Stroke Audit in the UK • 1997 Department of Health commissioned national stroke audit • Intercollegiate stroke working party • Audits conducted every 2 years • Structure • Process • (Outcome) • Patient experience (Picker survey) • Primary care audit • Now funded by HQIP
Features of Audit 1 • 100% participation • Run by clinicians • Exceptional level of data quality and completeness • Detailed analysis centrally to allow tailored interrogation of data • Performed every 2 years allowing time for implementation of change • Rapid production of results
Features of Audit 2 • Individual detailed hospital reports with results benchmarked against national/regional averages • Reports to Strategic Health Authorities, Healthcare Commission, Networks, Department of Health and Parliament • Extensive media coverage because public data of key indicators
Other sources of data • Primary care – Quality Outcomes Framework (QOF) • Vital signs data • Accelerated metrics for SIP • Routine Hospital Statistics (HES). Used by Dr Foster
Number of 9 Key Indicators Achieved Only 32% of patients who were eligible for all 9 indicators received all 9.
12 Key Process Indicators (2010) This round we have added four additional indicators and removed one (rehab goals agreed by discharge)
Number of 12 Key Indicators Achieved Only 16% of patients who were eligible for all 12 indicators received all nine.
How are the data used to influence change? • Workshops • Slide toolkits • Publicity • “I’ve been trying to get the trust to offer scanning for stroke patients for 5 years, within a day of receiving the audit report the chief executive had convened a meeting with stroke service and radiology” A stroke physician after publication of performance indicators 2004 audit • Influencing policy at a national level • Influencing policy at SHA level
Transforming Stroke care in London:Case for change London Stroke Providers against Sentinel Audit 12 key indicators 2006 Change in London Stroke Providers against Sentinel Audit 12 key indicators 2006 vs 2004 scores London Stroke Units Sentinel Audit Comparison 2004 and 2006 • Above Target Below Target Target 90
The scale of the problem of stroke in London • Second biggest killer and most common cause of disability • Population >8 million • 11,500 strokes a year in London – 2,000 deaths
30-minute blue light ambulance travel time from the hyper-acute stroke units The green area shows the areas that are within 30 minutes travel time (under ambulance blue light conditions) of a proposed HASU
London Stroke Strategy • Additional £20m per year for stroke care but only paid if hospitals delivering the required quality • Centralise hyperacute (hyperacute stroke units HASU) care into 8 units situated to provide easy access to the whole population (no more than 30 minutes by ambulance) • All acute stroke patients admitted to HASU. This is not just a thrombolysis service • Further 20 stroke units for on going rehabilitation • Improve community care and longer term rehabilitation • Neurovascular services for patients with TIA
London SHA Stroke Strategy • Bidding process to provide care • London Clinical Director • Regular inspections to ensure quality of care maintained • Obliged to submit continuous audit
Prophets of Doom Predictions • Not possible to implement major system reorganisation in London for a condition as complex as stroke • Staffing requirements unachievable (400 nurses and 100 therapists) • Recruitment – where will staff come from? • Training – how will staff develop the necessary skills? • Leadership – who can provide the necessary leadership? • There is a risk that the available workforce will be consumed by early implementers, leaving later implementers unable to recruit to posts.
Prophets of doom predictions • Patients will not accept being taken to a hospital that is not local to them • Not possible to transport people within 30 minutes to a HASU • Repatriation will fail and HASUs will quickly become full • Even if get acute services working it will fail because impossible to change community services • Unsustainable
1 year outcomes % of patients spending 90% of their time on a dedicated SU
1 year outcomes Average length of stay
1 year outcomes Thrombolysis rates 14% 12% 10% 3.5% Jan-March 2011 Feb-July 2009 Aim Feb-July 2010
London Stroke Survival vs Rest of England Hazard ratio for survival in London 0.72 95%CI 0.67-0.77 p<0.001
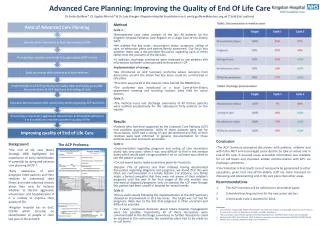
Cost-effectiveness analysis of the London Stroke Service:Results based on 6438 strokes per annum Professor Steve Morris et al
Cost-effectiveness analysis of the London Stroke Service:Results based on 6438 strokes per annum
Cost-effectiveness analysis of the London Stroke Service:Results based on 6438 strokes per annum
Results were qualitatively unchanged after undertaking sensitivity analysis on the following: Stroke mimics LOS in the HASU Unit cost per day in the HASU LOS in ICU Neurosurgery rates Discharge destinations Sensitivity analysis
Cost-effectiveness plane Costs (£) Higher costs Quadrant 1 Quadrant 4 CostBefore Before Quadrant 3 Quadrant 2 Lower costs Effects (e.g., deaths, QALYs) OutcomeBefore Worse outcomes Better outcomes
Cost-effectiveness plane Costs (£) Higher costs Quadrant 1 Quadrant 4 CostBefore Before Quadrant 3 Quadrant 2 Lower costs Effects (e.g., deaths, QALYs) OutcomeBefore Worse outcomes Better outcomes
Areas where work still needed • Early supported discharge • Bed based intermediate care • Longer term rehabilitation • Vocational rehabilitation
SINAP Click on the relevant number on the map or below to go to your region’s results 1North East 2North West 3 Yorkshire and the Humber 4West Midlands 5East Midlands 6East of England 7South West 8South Central 9London 10South East Coast 1 3 2 5 4 6 8 9 7 10