Download
1 / 22
220 likes | 542 Views
Modeling the Ebola Outbreak in West Africa, 2014. Sept 5 th Update Bryan Lewis PhD, MPH ( blewis@vbi.vt.edu ) Caitlin Rivers MPH, Eric Lofgren PhD, James Schlitt , Katie Dunphy , Stephen Eubank PhD, Madhav Marathe PhD, and Chris Barrett PhD. Currently Used Data.

E N D
Modeling the Ebola Outbreak in West Africa, 2014 Sept 5th Update Bryan Lewis PhD, MPH (blewis@vbi.vt.edu) Caitlin Rivers MPH, Eric Lofgren PhD, James Schlitt, Katie Dunphy, Stephen Eubank PhD, MadhavMarathe PhD, and Chris Barrett PhD
Currently Used Data • Data from WHO, MoH Liberia, and MoH Sierra Leone, available here: • https://github.com/cmrivers/ebola • Sierra Leone case counts censored up to 4/30/14. • Time series was filled in with missing dates, and case counts were interpolated.
Liberia Forecasts Forecast performance Model Parameters 'alpha':1/12, 'beta_I':0.17950, 'beta_H':0.062036, 'beta_F':0.489256, 'gamma_h':0.308899, 'gamma_d':0.075121, 'gamma_I':0.050000, 'gamma_f':0.496443, 'delta_1':.5, 'delta_2':.5, 'dx':0.510845 rI: 0.95 rH: 0.65 rF: 0.61 R0 total: 2.22
Forecasting Resource Demand • Accounting for prevalent cases in the model • Can include their modeled state: community, hospital, or burial • Help with logisitical planning
Exhausting Health Care System • Model adjusted to have limited capacity “better” health compartment (sized: 300, 500, 1000, 2000 beds) added to existing “degraded” health compartment (previous fit) • Those in new health compartment assumed to be • Well isolated and the dead are buried properly (ie once in the health system, very limited transmission to community 90% less than original fit) • More beds have a measurable impact in total cases at 2 months, but does not halt transmission alone
Next Steps • Agent-based modeling: • Initial version of Sierra Leone constructed • Need more work on mixing estimates • Initial look at sublocation modeling required a re-adjustment • Gathering data to assist in logistical questions • Further refinement of compartmental model to look at health-care system questions • Impact of increased / decreased effectiveness
Supporting material describing model structure, and additional results Appendix
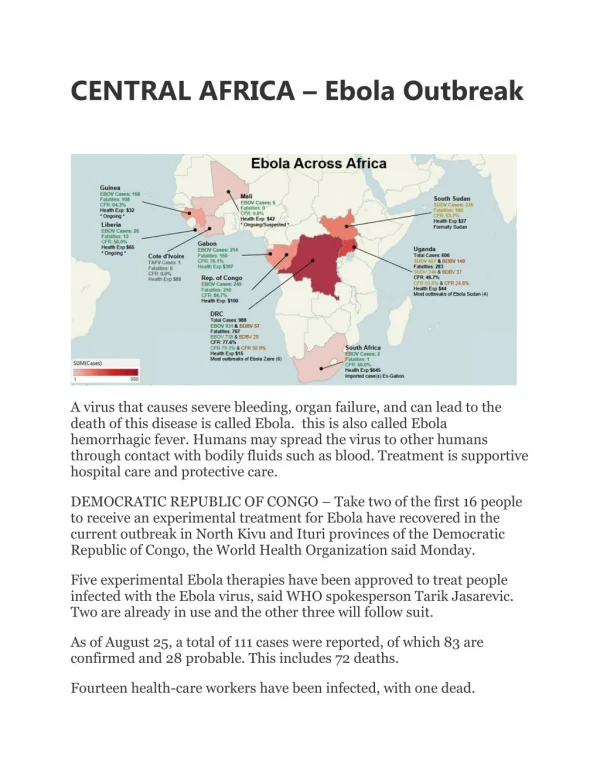
Epi Notes • Case identified in Senegal • Guinean student, sought care in Dakar, identified and quarantined though did not report exposure to Ebola, thus HCWs were exposed. BBC • Liberian HCWs survival credited to Zmapp • Dr. SengaOmeonga and physician assistant KyndaKobbah were discharged from a Liberian treatment center on Saturday after recovering from the virus, according to the World Health Organization. CNN
Epi Notes • Guinea riot in Nzerekore (2nd city) on Aug 29 • Market area “disinfected,” angry residents attack HCW and hospital, “Ebola is a lie” BBC • India quarantines 6 “high-risk” Ebola suspects on Monday in New Delhi • Among 181 passengers who arrived in India from the affected western African countries HealthMap
Further evidence of endemic Ebola • 1985 manuscript finds ~13% sero-prevalence of Ebola in remote Liberia • Paired control study: Half from epilepsy patients and half from healthy volunteers • Geographic and social group sub-analysis shows all affected ~equally
Twitter Tracking Most common images: Risk map, lab work (britain), joke cartoon, EBV rally
Legrand et al. Model Description Legrand, J, R F Grais, P Y Boelle, A J Valleron, and A Flahault. “Understanding the Dynamics of Ebola Epidemics” Epidemiology and Infection 135 (4). 2007. Cambridge University Press: 610–21. doi:10.1017/S0950268806007217.
Compartmental Model • Extension of model proposed by Legrand et al. Legrand, J, R F Grais, P Y Boelle, A J Valleron, and A Flahault. “Understanding the Dynamics of Ebola Epidemics” Epidemiology and Infection 135 (4). 2007. Cambridge University Press: 610–21. doi:10.1017/S0950268806007217.
Legrand et al. Approach • Behavioral changes to reduce transmissibilities at specified days • Stochastic implementation fit to two historical outbreaks • Kikwit, DRC, 1995 • Gulu, Uganda, 2000 • Finds two different “types” of outbreaks • Community vs. Funeral driven outbreaks
NDSSL Extensions to Legrand Model • Multiple stages of behavioral change possible during this prolonged outbreak • Optimization of fit through automated method • Experiment: • Explore “degree” of fit using the two different outbreak types for each country in current outbreak
Optimized Fit Process • Parameters to explored selected • Diag_rate, beta_I, beta_H, beta_F, gamma_I, gamma_D, gamma_F, gamma_H • Initial values based on two historical outbreak • Optimization routine • Runs model with various permutations of parameters • Output compared to observed case count • Algorithm chooses combinations that minimize the difference between observed case counts and model outputs, selects “best” one
Fitted Model Caveats • Assumptions: • Behavioral changes effect each transmission route similarly • Mixing occurs differently for each of the three compartments but uniformly within • These models are likely “overfitted” • Many combos of parameters will fit the same curve • Guided by knowledge of the outbreak and additional data sources to keep parameters plausible • Structure of the model is supported
Sierra Leone Forecasts rI:0.85 rH:0.74 rF:0.31 R0 total: 1.90 Model Parameters 'alpha':1/10 'beta_I':0.164121 'beta_H':0.048990 'beta_F':.16 'gamma_h':0.296 'gamma_d':0.044827 'gamma_I':0.055 'gamma_f':0.25 'delta_1':.55 delta_2':.55 'dx':0.58
All Countries Forecasts rI:0.85 rH:0.74 rF:0.31 Overal:1.90
Exhausting Health Care System • Model adjusted to have limited capacity “better” health compartment (sized: 300, 500, 1000, 2000 beds) added to existing “degraded” health compartment (previous fit) • Those in new health compartment assumed to be • Well isolated and the dead are buried properly (ie once in the health system, very limited transmission to community 90% less than original fit) • More beds have a measurable impact in total cases at 2 months, but does not halt transmission alone
Long-term Operational Estimates • Based on forced bend through extreme reduction in transmission coefficients, no evidence to support bends at these points • Long term projections are unstable