Download
1 / 73
740 likes | 941 Views
Biliary system. SHENG YAN MD. PhD. shengyan @zju.edu.cn Department of Hepatobiliary Pancreatic Surgery The First Affiliated Hospital. Anatomy of Biliary System. Methods of Investigation. Disorders of Gallbladder. Disorders of Bile Duct. Case discussion. 2. 3. 4. 5. 1.

E N D
Biliary system SHENG YANMD. PhD.shengyan@zju.edu.cn Department of Hepatobiliary Pancreatic Surgery The First Affiliated Hospital
Anatomy of Biliary System Methods of Investigation Disorders of Gallbladder Disorders of Bile Duct Case discussion 2 3 4 5 1
Pre-Test • Bile come from? • How bile was transported?
Secretion of Bile • About 75% bile was secreted from hepatocyte and 25% was produced by biliary epithelial. 75% 25%
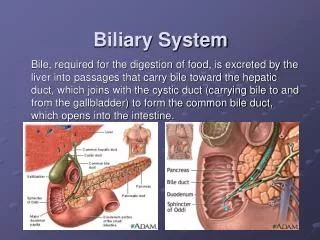
Anatomy of Biliary System Intrahepatic Biliary Tract Left Hepatic Bile duct Right Hepatic Bile duct Common Hepatic duct Cystic duct Common Bile duct
Anatomy of Biliary System Extrahepatic Biliary Tract Bifurcation Common hepatic duct Common bile duct Cystic duct Gallbladder
Calottriangle • The triangle is bounded by the cystic duct, the common hepatic duct, and the inferior border of the liver. • Important structures including: the cystic artery, the right hepatic artery, and the cystic duct lymph node.
The importance of Biliary system Achilles’heel In Greek mythology, when Achilles was a baby, it was foretold that he would die young To prevent his death, his mother Thetis took Achilles to the River Styx, which was supposed to offer powers of invulnerability, and dipped his body into the water. But as Thetis held Achilles by the heel, his heel was not washed over by the water of the magical river.
left hepatic artery right hepatic artery proper hepatic artery 3:00 artery 9:00 artery common hepatic artery retroduodenal artery gastroduodenal artery The importance of Biliary system The use of “Achilles heel” as an expression means “area of weakness, vulnerable spot”
Papilla of Vater • The opening of the bile duct and panceatic duct in the descending part of the duodenum. • Through the papilla, bile and pancreatic juice pass to bowel. • obstructive jaundice or pancreatitis will happen when papilla of Vater was blocked by stones and tumors,
Variations of biliary branching • A Typical anatomy of the confluence. • B Trifurcation of left, right anterior, and right posterior hepatic ducts. • C Aberrant drainage of a right anterior (C1) or posterior (C2) sectoral hepatic duct into the common hepatic duct.
Normal Gallbladder Gallbladder, with sludge and stone present
Multiple stones were found in the left intrahepatic bile duct.
MRCP showed slight dilation of CBD Pancreatic duct Common bile duct
Stones was detected in the bile duct by MRCP. Stones in CBD
ERCP Left: The endoscope was introduced to the papilla of Vater and contrast medium was injected into common bile duct. Right: Radiographic result after the contrast medium was injected into the CBD. • ERCP is the primary method of direct cholangiography, and has therapeutic potential. It also allows for examination of the upper GI tract, the papilla of Vater, and the pancreatic duct.
ERCP: Instruments can also be inserted through the scope to remove stones, insert stent, tissue biopsy, and other treatments.
PTC • The catheter was placed into the intrahepatic bile duct through patient’s skin guiding by B-US and fixed on the skin. • The radiographic image was taken. • Obstructive lesion can be seen in this picture.
Disorders of Gallbladder • Acute cholecystitis • Gallbladder stones and sludge • Adenomyomatous hyperplasia • Gallbladder polyps • Gallbladder carcinoma • ……
Acute Cholecystitis • Calculous cholecystitis: over 90% • Clinical manifestation: --Pain in right upper quadrant --Radiate to right shoulder & back --Nausea & vomiting --Chill and/or fever --Abdominal tenderness --Murphy's sign (+)
Murphy's sign • Ask the patient to breathe out • Then gently place the hand below the costal margin on the right side at the mid-clavicular line (the approximate location of the gallbladder). • The patient is then instructed to inspire (breathe in). During inspiration, the abdominal contents are pushed downward as the diaphragm moves down. If the patient stops breathing in (as the gallbladder is tender and, in moving downward, comes in contact with the examiner's fingers) and winces with a 'catch' in breath, the test is considered positive.
Acute Cholecystitis: B-US The gallbladder contains small stones in the neck and its wall shows edematous thickening (>5 mm thickness).
Gallbladder polyps • The majority of polyps are cholesterol • Cholesterol polyps are usually 2-10mm in size • They appear as small echogenic nonshadowing foci adherent to the gallbladder wall • Lack of mobility indicates polyp
Mirrizzi syndrome • Common hepatic duct obstruction caused by an extrinsic compression from an impacted stone in the cystic duct. • May result in biliary obstruction and jaundice • If not recognized preoperatively, it can result in significant morbidity and mortality
Open Cholecystectomy • The first case was performed in 1882 • One safe and effective method • Direct visualization and palpation
Gallbladder Carcinoma • Gallbladder carcinoma is associated with stones in over 90% of patients • There is a female to male ratio of 3:1 • Few patient was diagnosed prior to surgery
Gallbladder Carcinoma Cancer
Gallbladder Carcinoma Gallbladder Carcinoma Nodal Metastasis
Disorders of Bile Duct • AOSC • Choledocholithiasis/Hepatolithiasis • Choledochal cyst • Cholangiocarcinoma • Pancreatic and ampullary tumor
AOSC • Acute obstructive suppurative Cholangitis (AOSC) • Emergency disease carries high mortality • Common obstructing factors: stones, tumor • Complete obstruction and suppurative infection • May result in septicemia & septic shock; MSOF (multiple systemic organ failure)
Clinical manifestation Charcot triad • Abrupt onset ofpain in upper quadrant • Chill, high fever, may nausea and vomiting • Jaundice • May shock and altered mental status (Reynolds pentad)
Treatment • Correct the fluid and acid-base balance • Systemic administration of antibiotics • Anti-shock treatment • Drain the biliary tract: ERCP or PTCD • Emergency operation
ERCP: demonstrating stone in the duct (arrow) Choledocholithiasis/Hepatolithiasis Stones
Choledochal cysts • Cystic dilatation of the extrahepatic bile ducts • Female to male is about ration 4:1 • The majority are now diagnosed in childhood • Classified into five types • Associated with various biliary tumors