Download
1 / 1
10 likes | 99 Views
An Exploration of Insulin-like Growth Factor-1 Reference Ranges and Growth Hormone Deficiency: Who Are We Missing? Lisa Kreber, Ph.D.; Sarah Johnson, M.A.; Mark Ashley, Sc.D. Centre for Neuro Skills (CNS)-Clinical Research & Education Foundation (CREF). RESULTS:. BACKGROUND & SIGNIFICANCE:

E N D
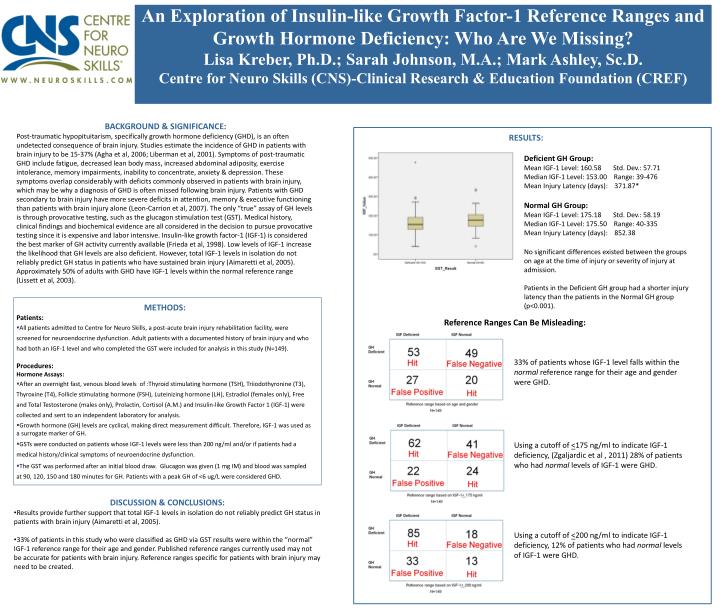
An Exploration of Insulin-like Growth Factor-1 Reference Ranges and Growth Hormone Deficiency: Who Are We Missing? Lisa Kreber, Ph.D.; Sarah Johnson, M.A.; Mark Ashley, Sc.D. Centre for Neuro Skills (CNS)-Clinical Research & Education Foundation (CREF) RESULTS: BACKGROUND & SIGNIFICANCE: Post-traumatic hypopituitarism, specifically growth hormone deficiency (GHD), is an often undetected consequence of brain injury. Studies estimate the incidence of GHD in patients with brain injury to be 15-37% (Agha et al, 2006; Liberman et al, 2001). Symptoms of post-traumatic GHD include fatigue, decreased lean body mass, increased abdominal adiposity, exercise intolerance, memory impairments, inability to concentrate, anxiety & depression. These symptoms overlap considerably with deficits commonly observed in patients with brain injury, which may be why a diagnosis of GHD is often missed following brain injury. Patients with GHD secondary to brain injury have more severe deficits in attention, memory & executive functioning than patients with brain injury alone (Leon-Carrion et al, 2007). The only “true” assay of GH levels is through provocative testing, such as the glucagon stimulation test (GST). Medical history, clinical findings and biochemical evidence are all considered in the decision to pursue provocative testing since it is expensive and labor intensive. Insulin-like growth factor-1 (IGF-1) is considered the best marker of GH activity currently available (Frieda et al, 1998). Low levels of IGF-1 increase the likelihood that GH levels are also deficient. However, total IGF-1 levels in isolation do not reliably predict GH status in patients who have sustained brain injury (Aimaretti et al, 2005). Approximately 50% of adults with GHD have IGF-1 levels within the normal reference range (Lissett et al, 2003). Deficient GH Group: Mean IGF-1 Level: 160.58 Std. Dev.: 57.71 Median IGF-1 Level: 153.00 Range: 39-476 Mean Injury Latency (days): 371.87* Normal GH Group: Mean IGF-1 Level: 175.18 Std. Dev.: 58.19 Median IGF-1 Level: 175.50 Range: 40-335 Mean Injury Latency (days): 852.38 No significant differences existed between the groups on age at the time of injury or severity of injury at admission. Patients in the Deficient GH group had a shorter injury latency than the patients in the Normal GH group (p<0.001). • METHODS: • Patients: • All patients admitted to Centre for Neuro Skills, a post-acute brain injury rehabilitation facility, were screened for neuroendocrine dysfunction. Adult patients with a documented history of brain injury and who had both an IGF-1 level and who completed the GST were included for analysis in this study (N=149). • Procedures: • Hormone Assays: • After an overnight fast, venous blood levels of :Thyroid stimulating hormone (TSH), Triiodothyronine (T3), Thyroxine (T4), Follicle stimulating hormone (FSH), Luteinizing hormone (LH), Estradiol (females only), Free and Total Testosterone (males only), Prolactin, Cortisol (A.M.) and Insulin-like Growth Factor 1 (IGF-1) were collected and sent to an independent laboratory for analysis. • Growth hormone (GH) levels are cyclical, making direct measurement difficult. Therefore, IGF-1 was used as a surrogate marker of GH. • GSTs were conducted on patients whose IGF-1 levels were less than 200 ng/ml and/or if patients had a medical history/clinical symptoms of neuroendocrine dysfunction. • The GST was performed after an initial blood draw. Glucagon was given (1 mg IM) and blood was sampled at 90, 120, 150 and 180 minutes for GH. Patients with a peak GH of <6 ug/L were considered GHD. Reference Ranges Can Be Misleading: 33% of patients whose IGF-1 level falls within the normal reference range for their age and gender were GHD. Using a cutoff of <175 ng/ml to indicate IGF-1 deficiency, (Zgaljardic et al , 2011) 28% of patients who had normal levels of IGF-1 were GHD. • DISCUSSION & CONCLUSIONS: • Results provide further support that total IGF-1 levels in isolation do not reliably predict GH status in patients with brain injury (Aimaretti et al, 2005). • 33% of patients in this study who were classified as GHD via GST results were within the “normal” IGF-1 reference range for their age and gender. Published reference ranges currently used may not be accurate for patients with brain injury. Reference ranges specific for patients with brain injury may need to be created. Using a cutoff of <200 ng/ml to indicate IGF-1 deficiency, 12% of patients who had normal levels of IGF-1 were GHD.