Download

1 / 31
330 likes | 593 Views
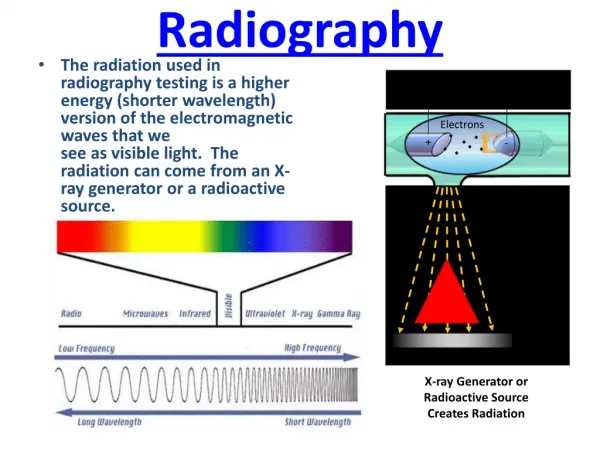
PEDIATRIC RADIOGRAPHY. The Role of The Radiographer in Dose Reduction for Paediatrics. Cynthia Cowling ACR, B.Sc. M.Ed Director of Education ISRRT Development Leader, Radiation Sciences Central Queensland University, Australia. 2. Outline. Traditional role and techniques

E N D
The Role of The Radiographer in Dose Reduction for Paediatrics Cynthia Cowling ACR, B.Sc. M.Ed Director of Education ISRRT Development Leader, Radiation Sciences Central Queensland University, Australia 2
Outline • Traditional role and techniques • Role in CT Dose Reduction • Implications for Interventional • Dose implications in the move from Analog to digital • Some specialized activities 3
The pediatric patient always presents with unique problems for the radiographer • Keeping still • Use of restraining devices • Response to verbal direction • Use of shielding • Role of the family
Use immobilization devices judiciously Capture the attention of the child 5
Other Devices • Tape (be careful not to hurt skin) • Sheets, towels • Sandbags • Radiolucient sponges • Compression bands • Stockinettes • Ace bandages
Radiation Protection • ALARA • Proper immobilization • Short exposure time • Limited views • Close collimation • Lead aprons and half shields
Differences children and adults • Mental development • Chest and abdomen the same circumference in NB • Pelvis - mostly cartilage • Abdominal organs higher in infants than older children • Hard to find ASIS or Iliac Crest in young child, can center 1 inch above umbilicus (bellybutton) • Exposure made as baby takes a breath to let out a cry
Dose reduction in CT Use Radiologists and radiographers must create an essential partnership It is the Radiographer who UNDERSTANDS and OPERATES the equipment All CT sites should cooperate; start reduction and validate results 9
Essential features • Dose should be age and weight specific • Dose should be customized to pathology • Number of follow ups should be scrutinized • Software features should be used if possible • Image enhancement • Modulation of mAs 10
Working with the radiologist, the radiographer… • Starts with standard protocol and then reduces to provide acceptable image • Screens all requests, re protocol and suitability of request • Attempts to narrow down area of interest 11
Interventional Procedures • Increased because of immediate risk benefit for child (not undergoing surgery) • However, not much consideration given to long term stochastic effects 12
Collaboration makes a huge difference • Example from Hospital for Sick Children, Toronto Canada • In Angio CT the TEAM was able to reduce dose from 3 mSev to 0.8 mSev as standard for typical Angio CT exam for child 13
Dose Optimization in CT • kVp – decrease kVp, decrease dose, increase image noise, non-linear • Ex. 140 kVp 80 kVp dose by 78% (Siegel M et al, 2004) • mAs – decrease mAs, decrease dose, increase noise, linear • Ie. Halve mAs, Halve dose • Pitch, length of scan, gantry cycle time
Cardiac Angiography CT Protocol • Weight-based protocol • IV injection of contrast • Set parameters: • Tube Voltage: 80 kVp • Gantry Rotation Time 0.4 s • Pitch 0.9 • Variable parameters: Vary mAs According to body weight • - <5 kg: 70 mAs [Newborn phantom] • - 5-25 kg: 80 mAs [1-, 5-year old phantom] • - 25-50 kg: 90 mAs [10-year old phantom] • - >50 kg: 100 mAs • Scan Coverage • Only area of interest
Conclusions New protocol/equipment exposes patients to less radiation than previous set-up Doses are less than 1 mSv across all phantoms ~75% decrease from previous protocol Images are of diagnostic quality Project is a good illustration of the utility we have at Sick Kids -> Easily determine radiation risk from various procedures with in-house equipment
Moving Forward • This study was a general view of the exam • Study Clinical assessments to: • Collect data on what scans are used to diagnosis for • Percentage diagnosis yield • Percentage of cases that would have benefitted from lower/higher dose • Can we tighten dose optimization further
EOS 1- Takes two simultaneous digital planar radiographs in the standing position with very low dose : 2D EOS 2D 2- Creates a three dimensional bone envelope weight bearing image : 3D sterEOS 3D
Scanning process Collimated detector Collimated X Ray beam scanning linear detector Linear scanning of a fan-shapedcollimated X ray beam from 5 cm to 180 cm (whole body) • No vertical divergence of X rays • No scatterdetect • SNR increased • Allows for lower dose ++
Dose & Image quality • Current practice : • - Scattered radiation accounts for more than 80% of the X-ray flux passing through the patient • - This noise reduces detectability and therefore a higher dose is required to maintain image quality • Clinical impact of dose : M. Doody et. Al., « Breast Cancer Mortality After Diagnostic Radiography », Spine, Vol. 25, No 16, pp 2052-2063 Retrospective study on mortality due to breast cancer (women followed for scoliosis using spine X-Rays) : • 5466 women followed between 1912 and 1965. Average of 25 radiographs (~0.11 Gy) • => Risk of death due to breast cancer is 69% higher than what is encountered in general population. • In a linear scanner such as EOS, the detector geometry prevents more than 99.9% of the scattered radiation from entering the detector • EOS allows for a dose reduction up to 10 times compared to CR 21
Dose reduction x9… …With improved or equivalent image quality (97%) High dynamic of image (16 bits, > 30 0000 Levels of Gray). Digital images, DICOM format Single exposure for multiple exams Pixel size 254µm EOS requires less dose (Montreal study on spine) 11% EOS Fuji 100% EOS lowers dose by over 89% Low dose & High Image Quality EOS Non EOS/Dose x10
Why Low Dose? • Slot Scanning Technology • No scatter detected, Noise suppressed • Allows for Lower Dose • Charpak Nobel Prize Winning Detector • Detector amplification : Photon gaz cascade, High gain signal, sensitivity maximized • Automatic internal gain adjustment • Dynamic range outperform other digital imaging technology (30,000 gray levels) • Available for any patient!
Analog to Digital, Dose implications • Requires changes to radiographer’s knowledge base • Radiographers work practicemust change to ensure high quality images • Must be more aware of dose since automation and image acquisition does not provide feedback in image production especially key effects of mAs and kVp • Radiographer must work as part of Team to ensure adherence to ALARA • QC always critical 24
Cont.. • Positioning can be more critical, aligning to detectors • Manual techniques may be required to produce optimum quality • Post processing as a method of enhancing image should be discouraged • Exposure creep must be avoided (any more than 4% unacceptable) ADVANTAGE provides statistical evidence of exposure factors and dose 25
How the profession can improve dose reduction • Increase awareness through membership in initiatives such as ImageGently • Provide retraining opportunities • Make use of publications such as ICRP • Participate in Clinical Audits • Actively work collaboratively with radiologists and physicians 26
For Example • In Ontario, Canada, Radiographers are regulated by the College of Medical Radiation Technologists of Ontario (CMRTO) and • Healing Arts Radiation Protection Act (HARP) which controls and identifies who can order and operate x ray equipment 27
Recommendations • HARP should require that prescribing or requesting a CT be permitted only by individuals who have appropriate clinical knowledge and training in radiation protection • All persons operating CT equipment or devices take a radiation safety course documented by a certificate of credentials • 200% increase in CTs in Ontario between 1996-2006 28
Enhancing Radiation Protection in Computed Tomography for Children Module two Image Gently www.imagegently.org 29
TWOKEYPOINTS TEAMWORK TRAINING TEAMWORK 30
Many Thanks and Acknowledgements to • Image Gently- Alliance for Radiation Safety in Pediatric Imaging • American Society of Radiologic Technologists-ASRT • Ellen Charkot, Director Imaging Services Hospital for Sick Children, Toronto Canada • Lori Boyd, Director of Policy College of Medical Radiation Technologists of Ontario, Canada (CMRTO) • Marie De La Simone, biospace med, Paris France • International Society of Radiographers and Radiological Technologists (ISRRT) • Maria del Rosario Perez, WHO 31