Download
1 / 24
240 likes | 448 Views
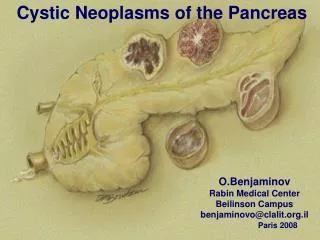
Cystic lesion of pancreas. Chan Chi King North District Hospital. The tumor, now the size of a small coconut , was a little above and to the left of the umbilicus, feeling like a tense cyst, & pulsating plainly form motion transmitted from the aorta. The dignosis of pancreatic cyst was made.

E N D
Cystic lesion of pancreas Chan Chi King North District Hospital
The tumor, now the size of a small coconut , was a little above and to the left of the umbilicus, feeling like a tense cyst, & pulsating plainly form motion transmitted from the aorta. The dignosis of pancreatic cyst was made.. Ann Surg. 1893 Aug;18(2):227-8
How common? • Prevalence 0.21% to 24.3% • Ikeda M. et al 1994; Kimura W. et al. 1995 • Size and number of pancreatic cysts increase with age Zhang. et al. 2002 • ? 80~90% pseudocyst • ? 10% cystic neoplasm • (1% of primary pancreatic neoplasm)
Cystic lesion of pancreas • A broad spectrum of pathological entities • Distinguish pancreatic pseudocyst/ non-neoplastic cyst from pancreatic cystic neoplasm • Distinguish benign cystic neoplasm from potential malignant cystic neoplasm
Non-neoplastic lesions Pseudocyst Inflammatory pancreatic cyst Simple epithelial cyst VHL Cystic fibrosis Neoplastic lesions Serous cystic neoplasm Mucinous cystic neoplasm Intraductal papillary mucinous neoplasm (IPMN) Cystic endocrine neoplasm Solid Pseudopapillary neoplasm Ducal adenocarcinoma with cystic degeneration Acinar cell cystadenocarcinoma
Epidemiology Brugge WR. et al.NEJM.2004.
Presentation • Found incidentally during imaging • Jaundice.. Abdominal pain.. weight loss.. Anorexia.. History of pancreatitis History of alcohol abuse History of abdominal injury Spinelli KS et al. Ann Surg.2004 Goh BK et al. Am J Surg.2006 Frenandez-del Castilo C et al. Arch Surg.2003 Allen PJ et al. J Gastrointest Surg.2003 >1/3 of Case Symptomatic cysts are associated with higher risk of malignancy ?Cofounding with increasedsize
Role of CT • Characterization of pancreatic cysts • May facilitate differentiation between histological variants for larger lesions • Remain non-diagnostic for small lesions • Firm diagnosis ~ 25 -40%
Microcystic Cyst with solid component Unilocular Cyst Marcocystic Dushyant V. Sahani et al. RadioGraphics 2005 Massachusetts General Hospital
Marcocystic lesion Mucinous cystic neoplasm
Role of MRI • Better delineate the architecture of cystic lesion • Better delineation of pancreatic duct • Not superior to thin cut CT in making diagnosis
Role of PET scan • Italian group at Padua Sperti C et al. J Gastrointest surg. 2005 • > 90% sensitivity / positive predicting value distinguish malignant from benign • Unable to distinguish pre-malignant from benign
Role of EUS morphologyaccuracy ~ 51% • Determine type and structure of cystic lesion • Facilitate fine needle aspiration • Examination of pancreatic ducts and parenchyma
Fine needle aspiratoncystic fluid analysis • Cytology • Tumor markers • CEA, CA19-9, CA 15-3, CA 72-4 • Amylase • Others
Small cystic lesions ( less than 3cm) • ~50% pre-malignant potential • ~ 13-20% malignancy ( < 3cm) • Resect or not to resect? • Surveillance? How? How Often? EUS/ CT Individualized decision Retrospective study Selection bias Overestimate the risk