Download
1 / 27
270 likes | 426 Views
Use of Routine Data to Monitor, Evaluate and Enhance Programs-- Swaziland. Wafaa El-Sadr, Velephi Okello, Margaret McNairy, Tanya Ellman, Altaye Kidane, Pido Bongomin, Harrison Kamiru, Jessica Justman and Ruben Sahabo ICAP at Columbia University and Ministry of Health in Swaziland.

E N D
Use of Routine Data to Monitor, Evaluate and Enhance Programs-- Swaziland Wafaa El-Sadr, Velephi Okello, Margaret McNairy, Tanya Ellman, Altaye Kidane, Pido Bongomin, Harrison Kamiru, Jessica Justman and Ruben Sahabo ICAP at Columbia University and Ministry of Health in Swaziland
Rapid Scale-Up of Treatmentin Swaziland Population: 1.2 million HIV Prevalence: 32% (18-49 y) (SHIMS 2011) HIV incidence: 2.4 per 100PY, (SHIMS 2001) Men: 1.7 Women: 3.1 Est. number of PLWH: 172,800 (2011) Facilities providing ART services: 134 Number on ART: 101,730 (2013) Adults 93,787 Children: 7,943 Ever enrolled on ART: 133,420
ICAP support for Swaziland Scale-up of Care and Treatment, 2009 to 2014 March 2014: 112 sites • Support for three of four regions: Hhohho, Manzini, and Lubombo • Technical assistance • National and site support • Health systems strengthening • Number of ART sites supported: 112 • Currently on ART: 73,737 • Ever enrolled on ART: 110, 351
Cumulative Number of Patients Initiating ART at ICAP-supported Sites, Oct 2009-Mar 2014: Swaziland 110,351 ByMarch 2014, 110,351 patients had ever initiated ART at ICAP-supported sites. 8% of patients were children 2010 2014
Ever attended HIV care among HIV-infected patients with CD4 < 350 SHIMS, 2012
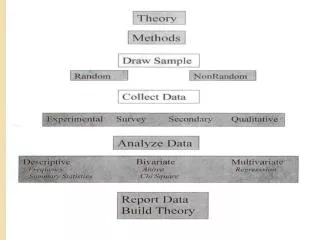
Approach to Address Gap in ART Initiations • Adapt a cascade approach to improve number of ART initiations • Identify baseline data to operationalize the cascade • Identify and prioritize interventions to address gaps • Identify priority sites • Introduce cohort methodology
1. Identify steps in the Relevant Cascade • Number of persons test HIV positive • Number of persons enroll in HIV care • Number of persons assessed for ART eligibility (WHO, CD4+ cell count) • Number of persons eligible for ART • Number of persons initiated ART
3- Choose and Prioritize Interventions: Focusing Matrix Ease of Implementation
Focusing Matrix Ease of Implementation # 2 priority most important and easiest to implement – #1 priority
Priority Interventions WHO Staging Tool • Universal assessment of ART eligibility: • Inconsistent use of WHO clinical staging • Job aide developed • Rapid turnaround of CD4+ cell count results • Peers (Expert Clients) review lab registers for CD4+ test results and call labs as needed • Scheduling of pre-ART patients for follow-up: • Document appointments for subsequent clinic visit and ART eligibility assessment • Peers make phone calls and if necessary conduct home visits for those who miss visits or unable to locate • Prompt ART initiation • Designate staff member to identify all ART-eligible patients not yet initiated ART and • place these patients’ folders in the “expected patient” box • Document the monthly number of ART-eligible patients yet to initiate • (goal of zero instituted) • On a weekly basis, peers and facility staff identify patients lost along the • cascade and call them for follow-up
4. Choosing Priority Sites Highest Volume Lowest Performance 65% 80% 42% 55% 30% 75% 20% 85% 66% 40% 35% 80%
4. Choosing Priority Sites Highest Volume Lowest Performance 65% 80% 42% 55% 30% 75% • 10 largest volume clinics in 3 regions = 30 sites • Volume defined by number of patients enrolling in HIV care in the past quarter 20% 85% 66% 40% 35% 80%
5. Introduce Cohort Methodology • Specify the best source of data for each step • Pre-ART register, patient HIV medical care file • Design simple tools (paper, Excel) for abstracting and summarizing these data • Excel sheet for data collection/management • Graph to display cascade data over time • Identify cohort members • Cohorts defined by month of pre-ART enrollment • Plan for periodic data collection • Establish team to review data and engage in action plan
Intervention roll-out begins Additional post-intervention cohort data to-be collected Baseline Cohort
89% 90% 92% 66% 62% 71%
Results of Interventions Proportion of Eligible Patients Initiating ART Increased from 63% to 81% • Efforts in Q4 resulted in an increase to 81% of eligible patients initiating ART by May • Findings from efforts informed target-setting for the following year
Maintenance of Targets • Since interventions implemented, continued success in reaching targets for ART initiations • In the first two quarters of following project year, 5,883 adults and children were initiated on ART – 95% of target ART Initiations, October 2013-March 2014
HIV Care Cascade Need for implementation science research to identify effective strategies McNairy, El-Sadr AIDS 2012
Implementation Science study • Aim: to improve linkage to care and retention in care • Objective: to evaluate the effectiveness of a combination intervention strategy of biomedical, behavioral and structural interventions • Anticipated Policy/Program implications: • Influence national policy recommendations for linkage and retention targets and interventions
HIV Care Cascade POC CD4 Package Of Care Rapid ART Initiation Financial Incentives McNairy, El-Sadr AIDS 2012
Conclusions • Enormous success has been achieved by Swaziland in the scale-up of HIV treatment • Routine data is of substantial value in informing progress, identifying gaps and guiding interventions • A step-wise process is critical to identify gaps, prioritize actions and measure outcomes • Engagement of teams of providers and supervisors at multiple levels is critical to achieve goals and objectives • Cohort approach allows for monitoring of progress • Implementation science research can inform program design and implementation through identification of innovative strategies for enhancing program outcomes
Acknowledgement • Support of the Ministry of Health in the Kingdom of Swaziland • Staff and patients at health facilities • Partner organizations • Funding support by PEPFAR