Download
1 / 53
3.52k likes | 7.5k Views
Health Care Financing. Health Care Finance. Definition : “ Function of a health system concerned with the accumulation , mobilization and allocation of money to cover the health needs of the people, individually and collectively, in the health system . ” (WHO). Purpose :

E N D
Health Care Financing www.powerppt.co
Health Care Finance • Definition :“Function of a health system concerned with the accumulation, mobilization and allocation of money to cover the health needs of the people, individually and collectively, in the health system.”(WHO) www.powerppt.co
Purpose : • Make funding available • Set the right financial incentives for providers • To ensure that all individuals have access to effective public health and personal health care. Health financing is raising of resources to support to pay for goods and health services. www.powerppt.co
Health Financing Mechanism • Health care financing is about 3 questions: • How is the money raised? • How are funds pooled? And • How are services paid for? • ANSWERS ARE : • Revenue Collection • Pooling • Purchasing of health services www.powerppt.co
1. How is the money raised ??? • Revenue collection : • 4 main ways of raising money for health care: • User pays (out of pocket, no reimbursement) • General Tax Revenue • Donor funding/Grants(external financing) • Health insurance contributions • Social health insurance • Private health insurance • Community based health insurance www.powerppt.co
2. How are funds pooled ??? Mobilization : • Accumulation & management of Revenue with respect to • Health Risk • Subsidy • Cross Subsidy • Pooling to redistribute health risk • Cross subsidy for greater equity www.powerppt.co
POOLING (Across equal income) CONTRIBUTION NET TRANSFER Low Risk High CROSS SUBSIDY (Across equal risk) Low Income High www.powerppt.co
3. How are services paid for ??? • Purchasing of health services : • It is done by public or private agencies that spend money either to provide services directly or to purchase services for their beneficiaries. • Purchaser : • Ministry of health (MOH) • Social security agencies • District health board • Insurance organization • Individual or household • Purchasing www.powerppt.co
Purchasing model It is based on the organizational relationships and contractual or purchasing relationships : • First model :where the government owns the buildings and employs the staff directly. • Second model: the patient provider contract, The patient pays the provider and then seeks re-imbursement from their insurer. • Third model:the purchaser provider contract, The provider have to provide services to the patient but the payment is paid by funder (Govt & insurer). • Fourth model: the patient pays the provider out-of-pocket and because the cost is not covered by insurer & it is not re-imbursable. www.powerppt.co
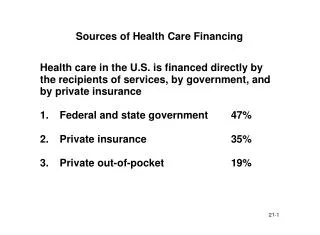
Patterns of healthcare financing across the world. Broadly, there are three patterns: • U.K- • The National Health Service (NHS) of the U.K. is a stark example of a state-run and publicly-funded system. The U.K. uses tax finances to pay for 80 per cent of its healthcare spending. • Europe- • Social insurance schemes bear most of the financial burden. • U.S.- • Relies on private insurance, paid for mostly by employers: almost half of the supersized health spending (16 per cent of GDP) is financed by tax money for the care of the old and the very poor. www.powerppt.co
HEALTHCARE FINANCE IN INDIA www.powerppt.co
Out of Pocket Payments (OOP) • Eg : User fees paid in hospitals. • Simplest form and common form. • OOP have two adverse consequences • Lower access to health care by creating financing barriers • impoverish the households because of high medical costs. www.powerppt.co
General Tax Revenue • Taxes – direct and indirect • The most equitable means for health financing. • Government health services are usually financed by general revenue sources www.powerppt.co
11th 5 yr plan- 83,407/- 12th 5 yr plan- 268,551/- www.powerppt.co
Comparison of GDP www.powerppt.co
Comparison of life expectancy at birth and GDP www.powerppt.co
Estimate of health expenditure in India 2004-05 to 2010 -11 www.powerppt.co
Comparison of GDP Lowest among BRICS Nations www.powerppt.co
GDP IN FIVE YR PLANS www.powerppt.co
Health expenditure per capita (US dollar) in India www.powerppt.co
Budget allocation in India • Allocation of money through five year plan • Annual allocation within the available five year funds. State Ministry of Finance (State have their own fund also) Ministry of health & FW Dept of health Other sector (Eg. Edu, social Welfare) MOH M of FW M of AYUSH Govt Health provider Private provider www.powerppt.co
Sharing Of Health Expenditure Between States And Centre www.powerppt.co
State Of Health Care www.powerppt.co
Health insurance • Mutual support system based on notion that “ I will help you in your current need , you to give me help when I need it. • Insurance : means it ensures every individual contributors that they don’t have to pay full cost of care out of pocket in the event of illness • 16 % population covered by any form of insurance. • Types: • Social health insurance • Private health insurance • Community health insurance www.powerppt.co
Social Health Insurance • Financed through payroll taxes, semi-autonomous administration, the care provided is through its own, public, or private facilities. • Strengths: • Additional health revenue source • Effectively redistribute between high and low risk and high and low income groups • Weakness: • High administrative cost. www.powerppt.co
POOLING (Across equal income) CONTRIBUTION NET TRANSFER Low Risk High CROSS SUBSIDY (Across equal risk) Low Income High www.powerppt.co
ESIS: • The Act compulsorily covers • All power using non-seasonal factories employing 10 or more persons • all non-power using factories employing 20 or more employees • Service establishments like shops, hotels restaurants, cinema, road transport and news papers. • Total beneficiaries: 6.63 crore • Doesn’t include people with wages > 15000 and also employees of Indian Air force, Navy, Army www.powerppt.co
CGHS: • Introduced in 1954 • Contributory health scheme • Approximately there are 5.5 million beneficiaries • ECHS: • For ex servicemen and there dependents • One time payment • Premium as per the rank www.powerppt.co
Social Health Insurance Schemes www.powerppt.co
Social Health Insurance Schemes www.powerppt.co
Social Health Insurance Schemes www.powerppt.co
Universal Health Insurance Scheme • Launched by Govt of India in 2003 • Standard medi-claim product with annual cover of Rs.30000 per annum. • Scheme targeted the BPL population Hence this scheme was superseded by RASTRIYA SWASTHYA BIMA YOJANA www.powerppt.co
RASHTRIYA SWASHTYA BIMA YOJANA • Started in April 2008 • Implemented in 25 states • Total sum insured is Rs. 30,000 per BPL family, with nominal registration fees as Rs. 30.00 • By 2011- 23 million families have enrolled. • Pre existing diseases are covered from day- 1 • Provision of smart card • Provision of transport allowance www.powerppt.co
RSBY Framework STATE GOVERNMENT STATE NODAL AGENCY CENTRAL GOVERNMENT PREMIUM – 25 % PREMIUM – 75 % INSURANCE COMPANY NGOs SMART CARD PAYMENT MANAGEMENT REGISTRATION COMMUNITY PROVIDERS CARE www.powerppt.co
Private Health Insurance • Voluntary health insurance scheme, with over 300 products from over 30 insurers competing in the market today. • Cover about 60 million people presently (excluding Government-funded schemes), roughly equally shared between Corporate (group) insurance plans and Retail (individual/family) plans. • TPA to facilitate speedier expansion by providing an administrative-intermediary. www.powerppt.co
Community Health Insurance • Any not for profit scheme aimed primarily at the informal sector and formed on the basis of collective pooling of health risks and in which the members participate in its management. • Initiated by NGOs. • 3 basic models • Provider model(direct model) • Insurer model(indirect model) • Linked model www.powerppt.co
Type I Provider + Insurer Community Type I: ACCORD, MGIMS, RAHA, SHH, VHS www.powerppt.co
Type II Insurer (NGO) Fees Provider Premium Care Community Type II: DHAN, Yeshasvini www.powerppt.co
Type III Insurer Company Premium NGO Provider Reimbursement Care Premium Community Type III: BAIF, KarunaTrust, SEWA www.powerppt.co
Yeshasvini • Organized by Yeshasvini trust, Karnataka • Eligibility : cooperative farmers & their families • Premium : Rs: 120 + 30 per person / yr • Benefit : any surgery up to 1 lakh per hospitalization & 2 lakh per patient / yr • Empanelled hospitals > 300 www.powerppt.co
Karuna Trust: • Initiated in September 2002 • Eligibility – BPL families in talukas where Karuna trust works • Premium – Rs 20 per person per year • Year Benefit – hospitalization expenses upto Rs 2500 • Payment to the doctors upto Rs 1500 • Providers – Only government hospitals www.powerppt.co
External funding www.powerppt.co
Recommendations • The future has to be tax funded. Preventive, primary and some part of secondary treatment has to be completely free, cashless and provided by the government and funded through taxes.” • Systems to track & audit expenditures against budget authorization • Community based research for credible burden of disease. www.powerppt.co
Develop public private partnership. • Increase spending on health promotion: 10%- 20% • Rationalizing & restructuring public health delivery system. • Integrating AYUSH-increase in human resource. • Raise additional resources by imposing taxes on health degrading products, eg, tobacco. www.powerppt.co