Download
1 / 10
100 likes | 211 Views
Prevention of SSI- Applying the Glucose Control Component Sharing the HHS Experience. Dr. Richard McLean, MD, FRCP(C) Emily Christoffersen RN, BScN Rhonda Smith RN, BScN, MEd. SSI project at HHS. Population: elective abdominal surgery patients at one site

E N D
Prevention of SSI- Applying the Glucose Control ComponentSharing the HHS Experience Dr. Richard McLean, MD, FRCP(C) Emily Christoffersen RN, BScN Rhonda Smith RN, BScN, MEd
SSI project at HHS • Population: elective abdominal surgery patients at one site • Bundle of three strategies: glucose control, maintenance of patient temperature, optimal antibiotic delivery • Dates: October 2004- present
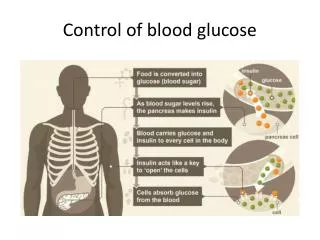
Why Glucose? • Diabetes an independent risk factor for infection in Cardiac Surgery Population [Harrington et a Infection Control and Hospital Epidemiology 2004] • New Hyperglycemia marker of poor clinical outcome: increased mortality/LOS/ICU Admission [Umpierrez J Clin Endocrinol Metab 2002] • Early Postoperative Hyperglycemia increases risk of nosocomial infection 5.9 fold [Pomposelli et al. Journal of Parenteral and Enteral Nutrition 1998] • Glucose control improves outcome in ICU population and in Cardiac Surgery [Van Den Berghe et al. NEJM 2001, Furnary et al Ann Thorac Surg 1999]
Change Concept: Develop your team • Identify project leaders (physician champion) • Outline roles • Engage frontline clinicians • Involve a multidisciplinary team (physicians/nurses/pharmacy) • Include members from all areas of care- preop, OR, PACU, post op units Need users of process to make improvements- helps with uptake
Change Concept: Create vision and commitment • Present literature about glucose control and SSI • Identify goals for caring for surgical patients re. glucose control Helps identify rationale- makes it real
Change concept: Outline current reality • Determine how currently monitor and treat glucose levels in surgical patients • Map-out processes • Involve all parts of care [preop clinic/same day surgery/operating room/PACU/Ward/ICU] Identifies where the group should start- what works well? what needs to change?
Change Concept:Design new processes • Identify processes for both monitoring and treatment • Developed preprinted orders • Developed standard documentation to follow through care process • Use rapid tests of change- plan, do, study, act • Simulate new process before implementation • First run with team involved in develpment • 2nd run “naive” team Build process with an eye on sustainability
New Process at HHS- Perioperative Glucose Control • All patients have CBG drawn in pre op clinic • Diabetics, and anyone with a random CBG >11 mmol will be flagged to have a repeat CBG day of surgery • These patients need CBG every two hours • CBG >11 in SDS or anytime during operative period- notify anaesthesiologist or surgeon • Transition to new subcutaneous insulin protocol post operatively as needed
What we’ve learned • Intervention needs to be tailored to patient population • What is the incidence of diabetes in the patient population? • Need a critical mass of patients to support insulin infusions in perioperative period • Be flexible- even if a new process is developed, be willing to change before full implementation • Must have lots of energetic, committed clinicians involved • Start developing preprinted orders as soon as possible