Download
1 / 22
230 likes | 449 Views
Pharmacogenetics of Antipsychotic Drug Response . Anil K. Malhotra, M.D. Zucker Hillside Hospital Glen Oaks, NY Albert Einstein College of Medicine Bronx, NY. Schizophrenia.

E N D
Pharmacogenetics of Antipsychotic Drug Response Anil K. Malhotra, M.D. Zucker Hillside Hospital Glen Oaks, NY Albert Einstein College of Medicine Bronx, NY
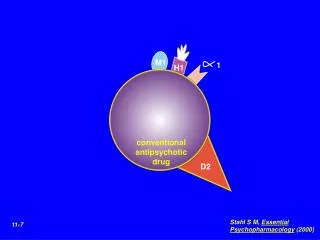
Schizophrenia • Chronic mental illness characterized by perceptual abnormalities, disorganized behavior, interpersonal problems and cognitive impairment • Affects approximately 1% of population worldwide • Associated with high levels of morbidity and mortality; 10% suicide rate in schizophrenia • Mainstay of treatment is the antipsychotic drugs
Discontinued Due to Lack of Efficacy Chouinard et al 1993 Marder & Melbach 1997 Beasley et al 1996 Tollefson et al 1997 Arvinitis et al 1997
Clinical Response over 4 Weeks of Antipsychotic Drug Treatment
Meta-analysis of Weight Gain Following Antipsychotic Drug Treatment
ALOX5 Genotype and Response to Antiasthma Treatment P <0.001 P = 0.026 P = 0.004 P = 0.039 FEV1 %ChangeFromBaseline
Pharmacogenetics of Clozapine Response Candidate Frequency of Association With Receptor Polymorphism Rare Allele Clozapine Response? D3 Ser9Gly 35% Yes (Shaikh et al, 1996) No (Malhotra et al, 1998) D4 16 amino acid repeat multiple alleles No (Rao et al, 1994) in exon III 5HT2A T102C 45% Yes (Arranz et al, 1996) No (Malhotra et al, 1996) His452Tyr 9% No (Malhotra et al, 1996) 5HT2C Cys23Ser 13% (males) Yes (Sodhi et al, 1995) 24% (females) No (Malhotra et al, 1996) 5HTT 20-34 bp repeat in 40% No (Arranz et al, 2000) 5 regulatory region
D2 Receptor Gene Polymorphisms • No common coding region polymorphisms (Gejman et al, 1994) • Two common SNPs, -141C Ins/Del and A241G, in promoter region (Arinami, et al, 1997) • -141C Ins/Del associated with schizophrenia (P <0.001) in a case-control study (N = 260) of Japanese patients
Functional Effects of the DRD2 -141C Ins/Del Polymorphism Transient expression of luciferase enzymatic activity driven by the DRD2 5’-flanking 304 bp containing the A-241 and -141C Del alleles, the A-241 and -141C Ins alleles in Y79 (A) and 293 (B) cells P <0.02 P <0.01 Percentage From Arinami et al, 1997.
Pharmacogenetics of Clozapine Response: Methods • 72 DSM-IIIR diagnosed schizophrenic or schizoaffective patients (52M, 20F, age = 37.2 ± 7.5 years) from the NIMH and MPRC • BPRS ratings after 10 weeks of clozapine treatment (dose = 405 ± 125 mg/d) • Data analysis • Responder/nonresponder analysis • Comparison of BPRS score by genotype after clozapine treatment
-141C Ins/Del and Clozapine Response Clozapine Clozapine Responders Nonresponders Total Genotypea Del+ 2 (10%) 19 (37%) 21 (29%) Del- 19 (90%) 32 (63%) 51 (71%) Total 21 51 72 Alleleb Del 2 (5%) 20 (20%) 22 (15%) Ins 40 (95%) 82 (80%) 122 (85%) Total 42 102 144 aFET, P = 0.015 bFET, P = 0.023
DRD2 -141C Ins/Del and Clozapine Response 45 40 BPRS Total 18 Del+ 35 Del- 30 25 Typical Neuroleptic Clozapine
Association of 5-HT2C -759C/T Polymorphism and Weight Gain • Genotype was significantly associated with the increase in BMI • after 6 weeks (p<0.001) • and 10 weeks (p<0.001) • The association between genotype and weight gain at six weeks remained in: • males (p<0.01), • females (p<0.01) and in patients receiving only: • chlorpromazine (n=69, p<0.01), • risperidone (n=46, p<0.05) Change in BMI (kg/m2)
Association of 5-HT2C -759C/T Polymorphism and Weight Gain Patients with clinically significant weight gain: (increase of >7%) • At six weeks27/96 (28%) wild-type and 0/27 (0%) variant cases (p=0.002) • At ten weeks46/90 (51%) wild-type and 4/27 (15%) variant cases (p=0.001) Odds ratio = 6.0 Patients with –759C allele were far more likely to develop significant weight gain (relative risk 3.45) than those with the –759T allele.
New Developments in(Pharmaco)Genomics • Human genome sequence • Massive SNP identification efforts by industry and academia • New genotyping technologies in biotech (Affymetrix, Sequenom, Orchid…) • Currently, ~ 40 c/SNP genotype • Genomic control approaches
Case-Control Association Drug Responders Drug Non-Responders Measure allele frequencies in both samples, search for statistically significant differences
Transmission Disequilibrium Test (TDT) AB AC AB AE AE AE AB AC
Power of Case-Control vs Family-Based Association Genetic Model Allele Frequency Case-Control Family-Based Dominant 0.05 207 314 0.20 158 224 0.70 2,204 2,913 Recessive 0.05 28,820 38,909 0.20 712 972 0.70 160 199 Additive 0.05 502 734 0.20 238 333 0.70 530 686 = 5 x 10-8. Power = 0.80. From Risch and Teng, 1998.
Number of Unlinked Markers to Detect Stratification 0.35 0.30 0.25 0.20 0.15 0.10 0.05 0.00 RR = 1 RR = 2 RR = 4 RR = 8 Probability 0 5 10 15 20 25 30 35 40 No. of Unlinked Markers
Whole Genome Association: A Plausible Strategy to Identify New Drug Targets? • 2 - 3 coding or promoter region SNP’s in every gene expressed in the CNS • 20,000 - 30,000 genes in the CNS • Case-control association: genomic control with unlinked markers, haplotype analysis • Genotyping costs • 50,000 SNPs • 1,000 patients from a clinical trial population • @ 40 c/genotype = $20,000,000 • @ 1 c/genotype = $500,000
Acknowledgments NIMH MPRC Zucker Hillside • Robert Buchanan • Pat Ball • John Bates • Janet Lavelle • Alan Mendelowitz • Donna O’Shea • Kamran Razi • John Kane • Caleb Adler • Alan Breier • Alan Clifton • Lisa Kestler • David Pickar • Walter Rooney NIAAA • David Goldman • Norio Ozaki • Chiara Mazzanti Funding: NIMH, NARSAD, Stanley Foundation, Pfizer Inc.