Download
1 / 49
490 likes | 501 Views
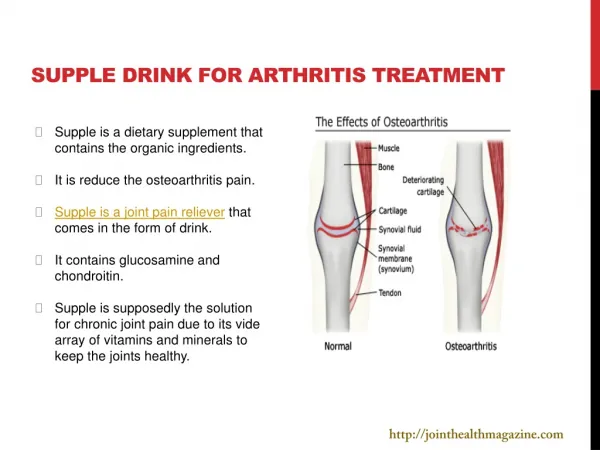
Microscopic evaluation of novel topical formulation for treatment of Arthritis. Mohit. CHITKARA COLLEGE OF PHARMACY CHITKARA UNIVERSITY, PUNJAB - 140401. INTRODUCTION. ARTHRITIS. Psoriatic Arthritis. Osteoarthritis. ARTHRITIS. Rheumatoid Arthritis. Joint Affected by Osteoarthritis.

E N D
Microscopic evaluation of novel topical formulation for treatment of Arthritis Mohit CHITKARA COLLEGE OF PHARMACY CHITKARA UNIVERSITY, PUNJAB - 140401
ARTHRITIS Psoriatic Arthritis Osteoarthritis ARTHRITIS Rheumatoid Arthritis Joint Affected by Osteoarthritis Psoriasis of Skin
ARTHRITIS(Cont…….) • Factors Involved in Autoimmune Disorders • Genetic disposition, • Environmental factors, • Endocrinological factors • Immune dysfunction • In indvidual with a susceptible genotype, exposure to above factors initiate an autoimmune response to self and foreign antigen through modulation of cytokines production and effector cell function
ETIOLOGY Immune System Gender • Unknown antigen initiates the immune response resulting in rheumatoid arthritis • Women get arthritis 2-3 times more often than men • Remission when they get pregnant. • Women have higher absolute number of CD4 lymphocytes relative to men,. ETIOLOGY Genetics Infection • Found in 20% of general population • Not a diagnostic tool, many people who have the marker either do not have or will never get rheumatoid arthritis. • Bacterial infections are most important eg. septic arthritis, reactive arthritis, osteomyletis and osteitis • Viral for eg. rubella virus, human parvovirus, hepatitis B virus • Fungal eg. Candida
DIAGNOSIS OF RHEUMATOID ARTHRITIS • PHYSICAL EXAMINATION • Joint swelling &tenderness • Malignancy • Loss of motion in joints MEDICAL HISTORY DIAGNOSIS • LAB TEST • Complete blood Count-Low WBC count suggests felty’s syndrome • Platelet count is elevatedin severe inflammation • Erythrocyte sedimentation rate (ESR) 60% of people have an elevated ESR • C-reactive protein • Rheumatoid factor (RF) +ive seropositive & -ive seronegative • Imaging studies Swelling of soft tissues and loss of bone density around the joints (X-ray) , MRI - Detect early inflammation before it is visible on X-rays, Joint ultrasound and bone densitometry -Measuring bone density used primarily to detect osteoporosis
CONVENTIONAL THERAPY • DMARD’S • Methotrexate (MTX) , Gold • Hydroxychloroquine • Sulfasalazine • Cyclosporine ,Azathioprine NSAID’S (Used in early weeks) Conventional therapy SYNOVIAL REPLISHNERS (Glucosamine ) BIOLOGIC RESPONSE MODIFIERS Remicade CORTICOSTERIODS Approved in 1996, Enbrel (etanercept) is the first biologic response modifier to receive FDA approval for patients with moderate to severe rheumatoid arthritis
LIMITATIONS OF ARTHRITIS THERAPY • NSAID’S About 80% of patient experience gastrointestinal side effect including gastric ulcer, perforation and hemorrhage etc • Colchicine Poor solubility leads to high variability in oral bioavailability (e.g. Celecoxib, Colchicine have variable oral bioavailability from 24 to 88%) Short biological half life (e.g. Colchicine has only 20 min.) • Systemic side effects High systemic side effects (e.g. Rofecoxib showed cardiotoxic and renal side effects leading to its withdrawal from market, Methotrexate has shown prominant hepatotoxic and bone marrow depression • Cost High cost of treatment (e.g. Methotrexate and TNF-α) Every year 1.5% of patient with rheumatoid arthritis are hospitalized with gastrointestinal problems
PROBLEMS IN PRESENT CONVENTIONAL THERAPY Several dose dependent toxic effect Can’t maintain a constant plasma level Short biological half life Also affect normal cells of body Low oral bioavailability Decrease efficacy of dugs during chronic use Conventional therapy Cost of treatment is high Minimum patient compliance
ADVANTAGES OF TOPICAL DRUG DELIVERY • Deliver a steady state infusion for prolong period of time • Reduce the adverse effect and toxicity • Improve the therapeutic utility of drug by reducing the problems like • First pass metabolism • GI irritation • GI decomposition • Low absorption • Increase the half life of drug • Reduce the frequency of administration • Improved patient compliance • Self administration is possible • Drug input can be terminated at any time
STRUCTURE AND FUNCTION OF HUMAN SKIN • Most extensive organ of body covering area of 2 m2 . Receive approximately one third of blood supply • For the purpose of transdermal/topical drug delivery, we can examine the structure and function of human skin categorized into four main layers: • Stratum corneum (Stratum corneum is the rate limiting barrier) • Epidermis • Dermis • Hypodermis
PROBLEM IN PRESENT ANTI-ARTHRITIC THERAPY AND PROPOSED STRATEGY FOR SITE-SPECIFIC DRUG DELIVERY Carrier
ELASTIC LIPOSOMES/ FATTY ACIDS AS CARRIER SYSTEM Lipid Bilayers • Modified lipid carriers that enable drug to reach deeper skin layers. • Colloidal particles, typically consisting of phospholipids and surfactant molecules. • Pass through skin pores of size less than their own diameter. • Serve as rate limiting membrane barrier for systemic absorption of drugs. • Accommodate both hydrophilic and lipophilic drugs. • Liposomal surfactants are biodegradable and biocompatible. • Prolong the drug release. Aqueous Cavity
IN VIVO MODELS FOR ARTHRITIS Antigen-Adjuvant induced model for arthritis Intraarticular injections of soluble antigen (same mice previously immunized to the same antigen ) Water in oil emulsion by combining one volume of FCA with one volume of aqueous antigen solution Acute arthritis Interaction with relevant cells • FCA enhances antibody production primarily because of the depot effect • Nonspecific immunopotentiation of macrophages by surfactant and the mycobacterium The adjuvant is a mixture of non-metabolizable oil (mineral oil), a surfactant (Aracel.A) and mycobacterium (M.tuberculosis or M.butyricum) is considered to be one of the most effective adjuvant
DRUG INTRODUCTION Chemical structure of methotrexate • Methotrexate (MTX) is a folic acid antagonist preferably used for long-term therapy of rheumatoid arthritis • Available in oral tablet and injectable form • Poor bioavailability &systemic use of this drug may provoke any of a number of side effects mainly hepatotoxicity and bone marrow suppression agranulocytosis and thrombocytopenia
DRUG INTRODUCTION Chemical structure of glucosamine • The daily oral dose requirement of glucosamine is 1500mg/day • Available in oral tablet and injectable form • Oral bioavailability of drug molecule is just 26%(subjected to uptake and degradation by the liver ) A major problem in topical administration of these proposed drugs is its hydro-solubility and dissociation at physiological pH so its capacity for passive diffusion is thus limited.
ARTHRITIC DRUGS MARKET The major players in the arthritis drug market include Abbott Laboratories Johnson & Johnson Amgen Roche Pfizer As of 2008, Abbott Laboratories' Humira, which was approved by the FDA in 2003, is the highest selling drug in the arthritis market, with sales growing 50% from 2007 to 2010 to $8.5 billion
THE OBJECTIVES OF THE PROPOSED RESEARCH WORK To develop novel drug delivery system, which provide sustained and targeted delivery of DMR’D to their target site (joints). To prepare, characterize and optimize different vesicular formulations(,fatty acid vesicles, Niosomes, elastic liposomes) To carry out stability and skin permeation studies of optimized vesicular formulation. To compare in vivo anti-arthritic activity of developed vesicular formulations with marketed formulation.
METHODLOGY • Identification and characterization of drug • Estimation of drugs in buffers and biological fluids by spectroscopy • Preparation of proposed vesicular system • Microscopic studies and characterization of proposed system • Phase contrast microscopy • Transmission electron microscopy • Scanning electron microscopy In vitro characterization of vesicular system • Shape • Size and size distribution studies ( Dynamic light scattering methods) • Entrapment efficiency (Minicolumn centrifugation methods) • Degree of deformability (Extrusion method)
METHODLOGY(cont….) • Zeta potential ( Zeta meter) • Turbidity measurement (Nephalometer) • No. of vesicles per cubic mm (Hemocytometer) • Phospholipid-ethanol interaction study (Differential Scanning Calorimetry) • In vitro skin permeation and deposition study (Using Diffusion Cell) • Stability study of the optimized formulation • In vivo study • Fluorescence microscopy of rat viable skin to determine the extend of penetration of vesicular formulation (Qualitative) • Confocal laser scanning Microscopy (CLSM) of rat viable skin to determine the rate and extend of penetration (Quantitative) • Histopathological study of inflamed joint
IMPORTANCE OF PROPOSED RESEARCH INVESTIGATION (National &International market status…) • Prevalence of arthritis in India increased drastically for last one decade • Dramatic increase in the demand of anti-arthritis drug • The market for rheumatoid arthritis therapeutics is estimated to reach over $20B in 2011 • Proposed novel formulations will selectively deliver the drug to thetargeted inflamed joint • Naturally taken up by cells of mononuclear phagocytic system(MPS) • Biocompatible and biodegradable as they are made from natural phospholipid • Reducing the dose of the drug by minimizing the systemic exposure of drug and increasing the deposition in deeper layer of skin • Easy to scale up, as procedure is simple, do not involve lengthy procedure and unnecessary use of pharmaceutically unacceptable additives
EXPERIMENTAL WORKDONE • IDENTIFICATION (Drug selected for study) • Ultraviolet Absorption Maxima (Max) Methotrexate and glucosamine :- 100µg /ml stock solution in distilled water Scanned:- Between 200-400nm exhibits maxima at 267 nm Results are concordant with the value given in the official books (Merck Index, 1996). • Infrared Spectral Assignment The IR spectra of MTX was recorded using (Perkin Elmer, IR Spectrophotometer). • Nuclear Magnetic Resonance The NMR spectra of MTX was recorded using (Bruker, NMR).
PREFORMULATION STUDIES SOLUBILITY STUDIES PARTITION COEFFICIENT Table :- Partition coefficient data of MTX Table :- Solubility Profile of MTX in Different Solvents
PREFORMULATION STUDIES Table:- PREFORMULATION STUDIES
STANDARD CURVE OF MTX IN DISTILLED WATER BY UV SPECTROPHOTOMETRIC METHOD Table :- Standard Curve of MTX In Distilled Water at Max 302 nm
STANDARD CURVE OF MTX IN PBS (pH 7.4) BY UV SPECTROPHOTOMETRIC METHOD Table :- Standard Curve of MTX in PBS (pH 7.4) at Max 302 nm
HPLC ASSAY OF MTX Table :- Standard Curve of MTX in Distilled Water by HPLC Method
Fig.:- Standard Curve of MTX In Distilled Water by HPLC Method
DEVELOPMENT OF VESICULAR CARRIERS - BASIC PRINCIPLE Table1 Size and entrapment efficiency of the prepared oleic acid vesicles UF-1,2,3-ufasomes with different molar ratio of drug Liposomes Transfersomes PC + SURFACTANT PC + CHOLESTEROL Partially dehrdrate Skin surface Stratum corneum (15% Water) “Transdermal osmotic gradient” Dermal layer (75% Water) Transfersomes prevent complete dehydration Applied always nonocclusively Liposomes are less deformable therefore they dehydrate completely and fuse Due to deformability transfersomes pass through narrow pores in the skin Resulting in better skin permeation PC + SURFACTANT Fatty acid vesicles PC + FATTY ACID
VISUALIZATION OF ELASTIC LIPOSOMES TEM ( X 1,80, 000) Photomicrograph of liposomal formulation Optical microscopy ( X 450) Photomicrograph liposomal formulation
Figure - TEM Photomicrograph of UF-3 formulation of glucosamine
Size and entrapment efficiency of the prepared oleic acid vesiclesUF-1,2,3-ufasomes with different molar ratio of drug
Size and entrapment efficiency of the prepared oleic acid vesiclesUF-1,2,3-ufasomes with different molar ratio of drug
Fig. 2. Differential scanning calorimetry traces of oleic acid (a), oleic acid –MTX vesicles (b), oleic acid –MTX 8:2 vesicles (c) and oleic acid –MTX 9:1 vesicles (d).
A D B C Figure MTX UF-3 with different concentration of oleic acid
Optimized with span 20,conc of oleic acid 80%,ph 7.4,80mM B A figure –( A)-Optimized MTX, (B) Glucosamine ufasomal formulation
At different pH,conc of oleic acid 90% pH 5.5 pH 7.4 pH 8.5
pH8.5 pH 6.5 pH 5.5 pH7.4 Figure 4. Photomicrograph of oleic acid vesicles dispersion incubated at different pH (400× magnification).
Figure . Vesicle growth at low pH values 80mM concentration of oleic acid
Figure 15 Histological View of Saggital Section of Rat Knee Joint Samples.
Figure : Histological View of Saggital Section of Rat Knee Joint Samples.
Conclusion • The results of the present study demonstrated that proposed vesicular formulation possess great potential for skin accumulation, prolonging release, improving site specific delivery and reducing the skin toxicity of glucosamine and methotrexate . This formulation seems to represents an attractive strategy for site-specific sustained delivery of glucosamine and methotrexate. In addition they are cost effective and therapeutically viable. Sustained release behavior and drug retention in the deeper part of skin might be beneficial for the longterm effects of drugs. The oleic acid vesicles seemingly fuse with the skin and release the contents. They are seen to penetrate intact and to form drug depots in the skin. The fatty acid in addition may serve as a penetration enhancer, thus by circumventing the stratum corneum barrier potential they may lead to better permeation of the drug molecules.
Acknowledgement • Dr. Sandeep Arora, Director, Chitkara College of Pharmacy, Chitkara University, India • Dr Arvind Sharma, Associate Professor, Chitkara College of Pharmacy, Chitkara University, India