Download
1 / 22
230 likes | 409 Views
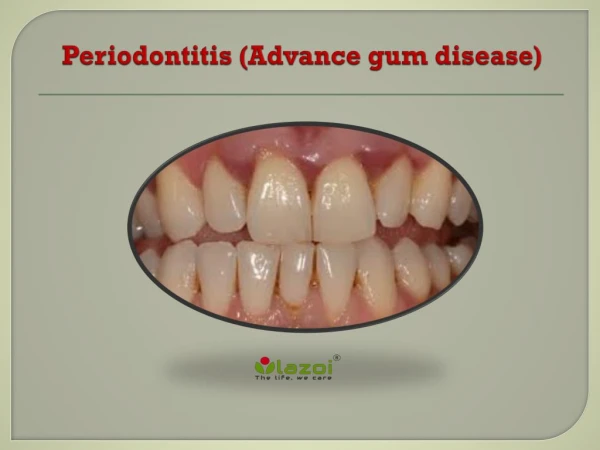
Periodontitis Acute periodontitis Acute inflammation of the perodontal ligament gradually involving the whole periodontium Causes (4I) Injury: trauma due to external force or bite on hard object Infection: Pulpitis, ANUG Irritation due to improper filling

E N D
Periodontitis Acute periodontitis • Acute inflammation of the perodontal ligament gradually involving the whole periodontium Causes (4I) • Injury: trauma due to external force or bite on hard object • Infection: Pulpitis, ANUG • Irritation due to improper filling • Impaction of foreign body (meat bone) • Etiological agent – Streptococcus, Staphylococcus, Borrelia vincenti • Fusiform bacillus Dr S Chakradhar
Clinical features • Toothache • Patient feels that the tooth is extruded • Fever • Malaise • Enlarged cervical LN Dr S Chakradhar
Management • Treat/remove the cause • Soft diet • Advise not to chew from affected side • Gargle with warm saline • Analgesics and anti inflammatory • Antibiotics • Prevent further damage by proper oral hygiene Dr S Chakradhar
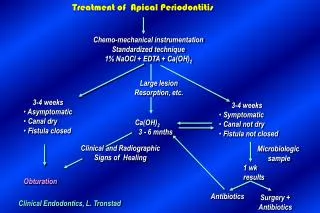
Periapical abscess • Usually a progression of periodontitis • History • Severe throbbing pain • Tenderness • Diffuse swelling • Fever
On examination • Inability to occlude • Fluctuant swelling in buccal or lingual region • Sensitive to percussion • Mobility • X ray may show periapical radiolucency
Management • Incision and drainage • Don’t give local infiltration as chances of dissemination of infection is there • Antibiotic coverage • Analgesic • Maintenance of oral hygiene
Chronic periodontitis • Causes • Chronic gingivitis • Occlusal trauma • Improper application of orthodontic appliance (excess force) Pathology • Destruction of periodontal ligament • Formation of periodontal pocket • Resorption of alveolar bone • Loosening of teeth
Clinical features • Features of chronic gingivitis • Swollen, soft, discolored • Bleeds on probing • Gingival pocket ( >4mm) • False pocket if gingiva is elongated towards crown. • Recession of gum margin • Mobile tooth • Halitosis
Management • Maintain oral hygiene • Brushing • Mouth wash • Scaling to remove plaque and calculi • Subgingival curettage of pocket, to allow normal reattachment of gingival and periodontal tissue • Mucogingival flap operation: curettage of granulation tissue, dead bone and cementum beneath a flap of gingiva
Complications • Intraoral and extraoral abscess • Maxillary sinusitis • Ostemyelitis of jaw • Cellulitis of face • Dissemination of infection: bacteremia, septicemia
Pericoronitis • Inflammation of the gingival tissue around an erupting tooth • When the eruption is partial, there is an opening through the mucus membrane and • rest of the crown is covered by a flap of gum which is known as operculum • Commonly occurs in the lower 3rd molar at the age of 18 to 25 yrs • But any tooth can be affected
Causes • Food stagnation and impaction • Upper tooth traumatizing lower gum flap • Vincent’s infection – acute gingivitis caused by borella vincemtis & fuscobacterium • Eruption irritation • Immunocompromised host
Clinical features • Pain • Swollen operculum • Trismus • Halitosis • Fever and enlarged cervical LN • Purulent exudate • Abscess formation
Management • Clean with 3%H2O2 • Nascent O2 is bactericidal • Normal saline wash • Maintain oral hygiene • Brushing • Antiseptic mouthwash • Chlorhexidine, Betadine, • Soft diet • Analgesic and anti inflammatory • Amoxycillin 500mg tds for 5 to 7 days Or Erythromycin 250mg qid for 5 to 7 days • Operculectomy • Removal of upper tooth may be necessary