Download
1 / 1
10 likes | 140 Views
Role of Subglottic Airway Narrowing in the Etiology of Obstructive Sleep Disordered Breathing in Non-Asthmatics. A.G. Sankri-Tarbichi 1,2 , S. Pranathiageswaran 1,2 , M.S. Badr 1,2 . 1 John D. Dingell VA Medical Center, Detroit, MI and 2 Wayne State University, Detroit, MI. INTRODUCTION.

E N D
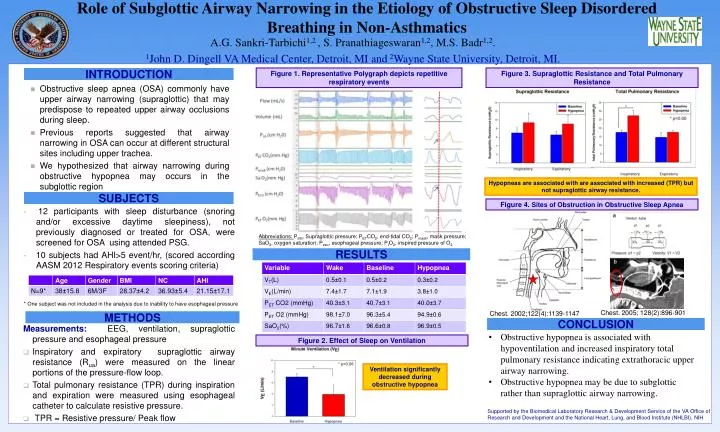
Role of Subglottic Airway Narrowing in the Etiology of Obstructive Sleep Disordered Breathing in Non-Asthmatics A.G. Sankri-Tarbichi1,2 , S. Pranathiageswaran1,2, M.S. Badr1,2. 1John D. Dingell VA Medical Center, Detroit, MI and 2Wayne State University, Detroit, MI. INTRODUCTION Figure 1. Representative Polygraph depicts repetitive respiratory events Figure 3. Supraglottic Resistance and Total Pulmonary Resistance • Obstructive sleep apnea (OSA) commonly have upper airway narrowing (supraglottic) that may predispose to repeated upper airway occlusions during sleep. • Previous reports suggested that airway narrowing in OSA can occur at different structural sites including upper trachea. • We hypothesized that airway narrowing during obstructive hypopnea may occurs in the subglottic region Hypopneas are associated with are associated with increased (TPR) but not supraglottic airway resistance. SUBJECTS Figure 4. Sites of Obstruction in Obstructive Sleep Apnea • 12 participants with sleep disturbance (snoring and/or excessive daytime sleepiness), not previously diagnosed or treated for OSA, were screened for OSA using attended PSG. • 10 subjects had AHI>5 event/hr, (scored according AASM 2012 Respiratory events scoring criteria) Abbreviations: PSG, Supraglottic pressure; PETCO2, end-tidal CO2; Pmask, mask pressure; SaO2, oxygen saturation; Peso, esophageal pressure; PIO2, inspired pressure of O2. RESULTS * One subject was not included in the analysis due to inability to have esophageal pressure Chest. 2005; 128(2):896-901 Chest. 2002;122(4):1139-1147 METHODS CONCLUSION • Measurements: EEG, ventilation, supraglottic pressure and esophageal pressure • Inspiratory and expiratory supraglottic airway resistance (Rua) were measured on the linear portions of the pressure-flow loop. • Total pulmonary resistance (TPR) during inspiration and expiration were measured using esophageal catheter to calculate resistive pressure. • TPR = Resistive pressure/ Peak flow • Obstructive hypopnea is associated with hypoventilation and increased inspiratory total pulmonary resistance indicating extrathoracic upper airway narrowing. • Obstructive hypopnea may be due to subglottic rather than supraglottic airway narrowing. Figure 2. Effect of Sleep on Ventilation Ventilation significantly decreased during obstructive hypopnea Supported by the Biomedical Laboratory Research & Development Service of the VA Office of Research and Development and the National Heart, Lung, and Blood Institute (NHLBI), NIH






















