Download

1 / 39
390 likes | 398 Views
Abnormalities of the testes and scrotum and their surgical management. Dr. S. Vahidi. Undescended testis Definition:. Testes located anywhere between the abdominal cavity and just outside the anatomic scrotum Abnormally position testis Cryptorchidism = hidden testis UDT Ectopic

E N D
Abnormalities of the testes and scrotum and their surgical management Dr. S. Vahidi
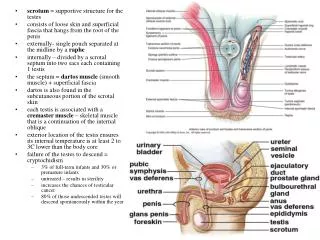
Undescended testis Definition: • Testes located anywhere between the abdominal cavity and just outside the anatomic scrotum • Abnormally position testis • Cryptorchidism = hidden testis • UDT • Ectopic • Un descended testis • Multiple etiologies diversity of this congenital disorders
Incidence • One of the most common congenital anomalies at birth • 3% of full-term male newborns • 1.6-1.9% unilateral • 30.3% in prematures • Preterm- low birth weight -twin - small for gestational age • 70-77% spontaneously descend, by 3 month. • 1% at 1 year of age
Epidemiology • Gestational age • Birth weight • Prematurity • Genetic- hormonal- environmental
Classification • Variation in testicular size & consistency • Epididymial & vassal anomalies • Patent processos vaginalis • Cryptorctidism: paplable- non palaplable: • Intra abdominal • Absent (vanishing) • Atrophic • Missed on Ph.E.
Cryptorchidism • Intra abdominal • Intra canalicular • Extra canalicular • Supra Pubic • Infra Pubic • Ectopic • Denis-browne pouch • Transverse scrotal • Femoral • Perineal • Prepenile
Retractile testis • Over active cremasteric reflex • Groin • 3-7 years of age • Infertility? • Delayed spontaneous T. Ascent
Theories of Descent & maldescent 3 phase of descending • Trans abdominal 23 week • Trans inguinal • Extra canalicular 23 week • Endocrine factors • Gubernaculum • Epididymis • Intra abdominal pressure • Histopathology
Endocrine factors Normal hypothalamic- pituitary-gonadal axis testicular descent • Androgenes: testosterone & DHT inguinal-scrotal phase of descent • Mullerian inhibiting substance (MIS)? • Estrogen? • Descendin: gubernacular specific growth factor
Gubernaculum • Major factor responsible for testicular descent • Physiologic mechanism? • Testicular descent: • Hormonal factors • Mechanical factors Genito femoral nerve and calcitonin Gene- related peptide?
Epididymis Epididymal abnormalities cryptorchidism Fertility in UDT • Germ cell development • EP. Anomalies
Intra abdominal pressure • Defects or agenesis of abdominal wall musculars UDT • Significant Role in trans inguinal descent
Histopathology • Leidig cells • Degeneration of sertoli cells • Delayed disappearance of gonocytes • Delayed appearavice of (Ad) spermatogonia • Failure of primary spermatocytes to develop • Germ cells • Similar pathology in the contralateral descended testis • < 2 years of age
Consequences of UDT • Infertility • Neoplasia • Hernia • Torsion
Consequences of UDT • Infertility • Bilateral or unilateral UDT • Early or delayed orchiopexy • Neoplasia • 10% of T. tumors arise from UDTs • T. tumors in UDT: 1/2550 • T. tumors in population: 1/100,000
Neoplasia (continued) • Presentation time: puperty • Orchiopexy affect the T. tumor? • The age of orchiopexy and T. tumor? • The location of T. & T. tumor • Seminoma is most common T. tumor • The cause of increased Risk: temprature or intrinsic pathologic process? • Routine T. biopsy during child hood orchiopexy?
Hernia • Patent processus vaginalis in >90% of UDT • Patent processus vaginalis affect the hormonal treatment of UDT T. Torsion
Work-up of UDT • 80% palpable • 20% non palpable • 20% absent • 30% atrophic • 50% intra abdominal
Work-up of UDT • History • Preterm H. • Perinatal H. • Past medical & surgical H. • Family H. • Ph.E • Other birth defect • Genital examination • Contralateral testis • Paraclinic • Accuracy of radiologic testing in UDT is 44% • Workup in Bilateral UDT • Hormonal workup (HCG stimulation test)- FSH- inhibin B- MIS
Management of UDT • Tenets of treatment • Proper identification of the Anatomy- position- viability • identification of coexisting syndrome • Placement of the testis within the scrotum • Permanent fixation and easy palpation • No further T. damage Definitive treatment should occur before 1 year of age
Indication for orchiectomy in UDT • Post pubescent males • Contralateral normal T. • Anatomically & morphologically abnormal • Too far from scrotum
Hormonal therapy • HCG • GnRH or LHRH • The lower position the better the success rate • Reascent in 25% of patient • Not indicated in: • Ectopic T. • Inguinal Hernia
HCG treatment • 14-59% success rate • 10,000 IU (1500 Iu/m2 im/2 week – 4 week) • Complications: GnRH • 19-32-65% success rate • 1.2 mg/day for 4 weeks. (nasal spray) Overall efficacy of hormonal treatment < 20% Surgery remains the Gold standard in the management of UDT
Surgical management of UDT • Standard orchiopexy • Ancillary techniques for the high UDT • Reoperative orchiopexy
Management of intra- abdominal testis • Laparoscopy • Fowler- stephenes orchiopexy • Microvascular auto transplantation Complications of orchiopexy
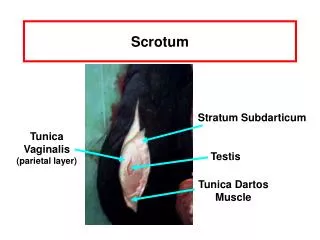
Hydrocele • Simple Hydrocele • Communicating Hydrocele • Hydrocele of the cord • Abdomino scrotal hydrocele
Acute scrotum • Acute scrotal pain – tenderness or swelling • Diff diagnosis
Torsion of the spermatic cord (intravaginal) • Golden time (4 hours) • Degree of torsion • Acute or gradual onset • Severe or minimized pain • Nausea & vomiting- the absence of cremasteric reflex • Manual detorsion • Doppler examination: false positive & false negative • Color doppler: 89% sensitivity 99% specifity? • Radinuclide imaging: sens 90% speci= 89%
Torsion (continued) • Explore Both side • Dartos pouch placement (no sutures) • Sympathetic orchiopathy?
Intermittent torsion • Torsion of the testicular and epididymal appendages • Perinatal torsion of the spermatic cord (extra vaginal) • No surgical exploration • Exploration of contralateral T.? • In postnatal torsion: exploration is needed (Bilateral)