Download
1 / 21
220 likes | 604 Views
Listeriosis. PREP, May 2004 Nelson, 17 th ED. Historical perspective. L. monocytogenous, why? Previously a rare cause of infection but today is isolated more frequently, why? Refrigerators. Highly processed food. Extended shelf life of foodstuffs.

E N D
Listeriosis PREP, May 2004 Nelson, 17th ED
Historical perspective • L. monocytogenous, why? • Previously a rare cause of infection but today is isolated more frequently, why? • Refrigerators. • Highly processed food. • Extended shelf life of foodstuffs. However it usually doesn’t cause disease.
Microbiology • Facultatively anaerobic G , non spore forming motile bacillus/ coccobacillus/ diplococci,or diphtheroids like. • It can tolerate low temperatures (4), high pH, high salt conc. So can replicate in soil, water, sewage, … & contaminated refrigerated foods. • Destroyed by pasteurization & most disinfecting agents.
Microbiology • L. monocytogenous is the commonest of the 7 species of the genus Listeria in causing disease. • On a semisolid media, demonstration of a tumbling motility, umbrella-type formation, hemolysis, & typical cAMP test are sufficient to establish a presumptive diagnosis of L mono.
Epidemiology • Important cause of zoonoses. • F- O transmission in animals. • Usually food- borne. • Animal to human by direct contact. • Vertical or horizontal transmission. • Cross- infection in a neonatal unit through contact with a contaminated mineral oil used to bathe infants.
Epidemiology • IP 3 weeks-30 days. • 5% of healthy adults have Listeria species in their stool (usually<1 mo). • Infectious dose 10*4- 10*6 / gram of ingested product & lower in special situations. • 0.7/100,000 general; 10/100,000 infants; 1.4/100,000 elderly. • Males more.
Pathogenesis • It causes granulomatous reactions & micro abscesses. • Translocations in animals. • It can cross the intestinal mucosal barrier & once in the blood stream, the bacteria may disseminate hematogenously to any site but mostly to the CNS or placenta, liver, & spleen.
Pathogenesis • It has the ability to escape from antibodies, complement, & neutrophils. • Intercurrent GI infection with another pathogen, as shigella sp., may enhance invasion in individuals infected with L monocytogenous. & it may enhance the transfer of intraluminal m.o across the intact intestinal mucosa.
Immunity • T cell mediated. • It is prevented through routine prophylaxis for Pneumocystis carinii in HIV patients. • Complement, opsonizing antibodies ?
Clinical Aspects • The enteric phase is usually asymptomatic, then the bacteria crosses the intestinal barrier to be transmitted inside the macrophages to any organ but mostly to the spleen & liver. • Disease & its severity depends on several factors.
Intrapartum Disease • Listeriosis in pregnancy: documented mostly in the 3rd trimester. Early: abortion. Second & third trimester: flu like illness or GI, rarely meningitis with/without fetal involvement ; stillbirth, premature labour (mortality rate 50- 90%). It may resolve after delivery even without treatment.
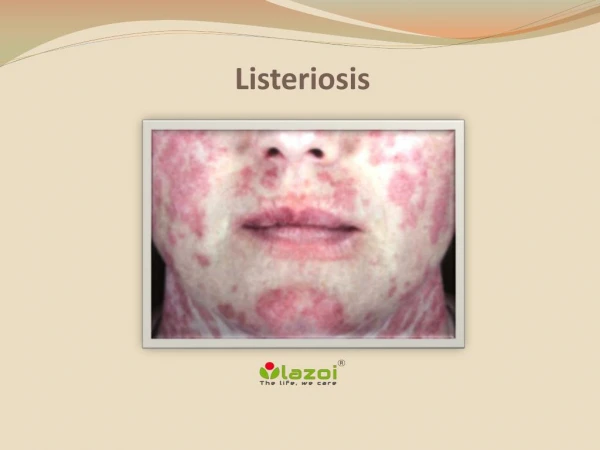
Neonatal DiseaseEarly Onset • 1.5 days (<5 days), mostly through the placenta (can be ascending). • Strong association with maternal disease. • Septic like picture predominates, but can be ARD, Pneumonia, Meningitis, Myocarditis. • Granulomatosis infantisepticum which are widely disseminated granulomas present in severe listerial disease (skin, liver, placenta).
Late Onset • Symptoms are several days to weeks after birth, usually at 14.3 days (5-30) of age. • Transmission is vertical or nosocomial. • Mostly as meningitis, in a term infant. • Less common. • Mothers are culture negative.
Nonperinatal Disease • Most common M.O as a cause of meningitis in patients with lymphoma, organ transplant recipients, in those receiving corticosteroids, & in the elderly. • Risk factors include DM., Liver disease, chronic renal disease, collagen vascular disease, iron overload, & diminished gastric acidity. However 54% of children have no apparent immunocompromising condition.
Nonperinatal Disease • After the neonatal period 30-55% present with meningitis. 30% will have neurologic sequelae (MR, hydrocephalus, e.t.c.) • Rhombencephalitis in healthy adults diagnosed by MRI. • Bacteremia in immunocompromised. • Infection in other body organs.
Diagnosis • It should be included in the differential diagnosis of infection in pregnancy, neonatal sepsis, meningitis. • CBC. • Gram stain. • Culture / 36 hr incubation/ blood, CSF, cervix, vagina, placenta. Alert the lab not to discard as a contaminating diphtheroids.
Diagnosis • CSF. Glucose, Blood Culture, Gram Stain, Protein. • Rapid detection by MA/ NAH. • PCR: not available commercially. • Anti-listeriolysin O, a hemolysin mediates lysis of vacuoles & is responsible for the zone of hemolysis when grown on blood containing solid media. • Serological test: not available. • Detect contact with animals.
Management • No available controlled trials about the exact drug or duration of treatment but a minimum of 2 weeks is needed. • Many factors make treatment difficult. • Antibiotics.
Prevention • Food-borne listeriosis: keeping uncooked meat separate from vegetables. Washing hands, knifes, & cutting boards after exposure to uncooked food. Regular cleaning & disinfection of the insides of refrigerators. At risk patients should avoid soft cheeses, reheat ( until steaming hot) leftover & ready to eat foods, avoid cold cuts if unable to reheat thoroughly.
Prevention • Zero tolerance policy. • Prophylaxis. • Vaccine. • It is a reportable disease.