Download
1 / 1
10 likes | 278 Views
Poster ID: CLP005. Melioidosis case report of a pediatric patient in Cambodia with extrapulmonary findings of mastoiditis and visceral abscesses Yos Pagnarith MD Angkor Hospital for Children (AHC), Siem Reap, Kingdom of Cambodia. Abstract

E N D
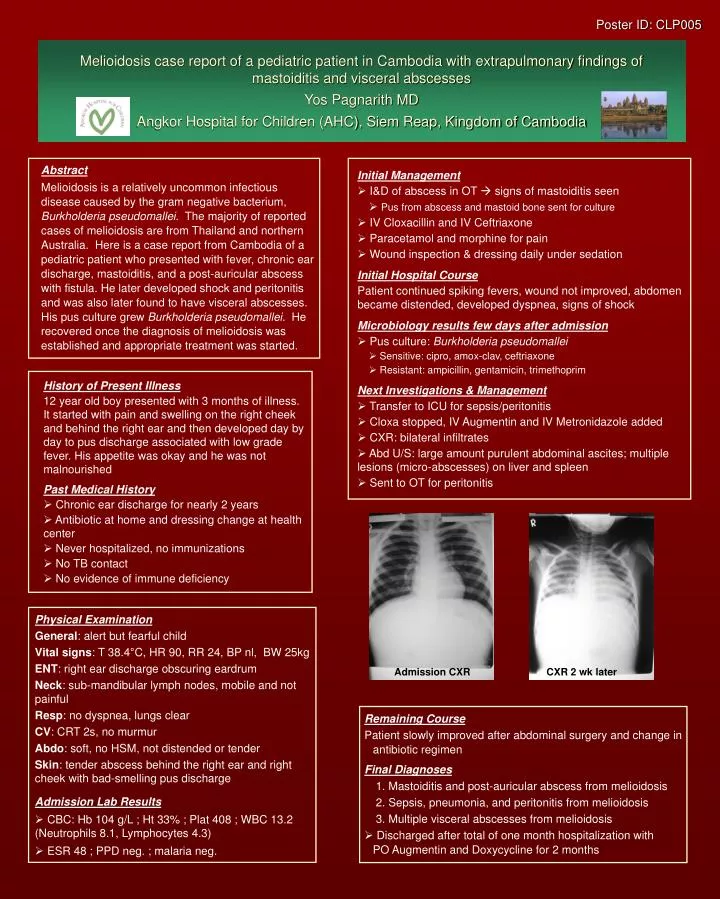
Poster ID: CLP005 Melioidosis case report of a pediatric patient in Cambodia with extrapulmonary findings of mastoiditis and visceral abscessesYos Pagnarith MDAngkor Hospital for Children (AHC), Siem Reap, Kingdom of Cambodia • Abstract • Melioidosis is a relatively uncommon infectious disease caused by the gram negative bacterium, Burkholderia pseudomallei. The majority of reported cases of melioidosis are from Thailand and northern Australia. Here is a case report from Cambodia of a pediatric patient who presented with fever, chronic ear discharge, mastoiditis, and a post-auricular abscess with fistula. He later developed shock and peritonitis and was also later found to have visceral abscesses. His pus culture grew Burkholderia pseudomallei. He recovered once the diagnosis of melioidosis was established and appropriate treatment was started. Initial Management • I&D of abscess in OT signs of mastoiditis seen • Pus from abscess and mastoid bone sent for culture • IV Cloxacillin and IV Ceftriaxone • Paracetamol and morphine for pain • Wound inspection & dressing daily under sedation Initial Hospital Course Patient continued spiking fevers, wound not improved, abdomen became distended, developed dyspnea, signs of shock Microbiology results few days after admission • Pus culture: Burkholderia pseudomallei • Sensitive: cipro, amox-clav, ceftriaxone • Resistant: ampicillin, gentamicin, trimethoprim Next Investigations & Management • Transfer to ICU for sepsis/peritonitis • Cloxa stopped, IV Augmentin and IV Metronidazole added • CXR: bilateral infiltrates • Abd U/S: large amount purulent abdominal ascites; multiple lesions (micro-abscesses) on liver and spleen • Sent to OT for peritonitis • History of Present Illness 12 year old boy presented with 3 months of illness. It started with pain and swelling on the right cheek and behind the right ear and then developed day by day to pus discharge associated with low grade fever. His appetite was okay and he was not malnourished Past Medical History • Chronic ear discharge for nearly 2 years • Antibiotic at home and dressing change at health center • Never hospitalized, no immunizations • No TB contact • No evidence of immune deficiency • Physical Examination • General: alert but fearful child • Vital signs: T 38.4°C, HR 90, RR 24, BP nl, BW 25kg • ENT: right ear discharge obscuring eardrum • Neck: sub-mandibular lymph nodes, mobile and not painful • Resp: no dyspnea, lungs clear • CV: CRT 2s, no murmur • Abdo: soft, no HSM, not distended or tender • Skin: tender abscess behind the right ear and right cheek with bad-smelling pus discharge • Admission Lab Results • CBC: Hb 104 g/L ; Ht 33% ; Plat 408 ; WBC 13.2 (Neutrophils 8.1, Lymphocytes 4.3) • ESR 48 ; PPD neg. ; malaria neg. Admission CXR CXR 2 wk later Remaining Course Patient slowly improved after abdominal surgery and change in antibiotic regimen Final Diagnoses • Mastoiditis and post-auricular abscess from melioidosis • Sepsis, pneumonia, and peritonitis from melioidosis • Multiple visceral abscesses from melioidosis • Discharged after total of one month hospitalization with PO Augmentin and Doxycycline for 2 months