Download
1 / 53
550 likes | 1.09k Views
Management of Gastroenteropancreatic Neuroendocrine T umour: a n update. Joint Hospital Surgical Grand Round Dr Chan Kwan Kit Caritas Medical Centre. Neuroendocrine Tumours (NETs). Epithelial neoplasms with predominant neuroendocrine differentiation

E N D
Management of Gastroenteropancreatic Neuroendocrine Tumour:an update Joint Hospital Surgical Grand Round Dr Chan Kwan Kit Caritas Medical Centre
Neuroendocrine Tumours (NETs) • Epithelial neoplasms with predominant neuroendocrine differentiation • Considered rare traditionally, comprising ~0.5% of all malignancies • Increasing incidence and prevalence, 2.5 -5/100,000 people per year • Increasing awareness • Improvement in diagnostic modalities
Distribution • Gastrointestinal tract: ~65% • Bronchopulmonary system: ~25% • Other locations ~10%: • thymus • gonads • heart • kidneys • prostate
Classifications • WHO classification: • tumour site • degree of differentiation and grading • functionality • TNM classification
Presentation • Asymptomatic • Non-functional: non-specific symptoms • abdominal pain, small bowel obstruction, gastrointestinal bleeding, anorexia, weight loss • Functional: hormone/ peptides-related • Serotonin: carcinoid syndrome • Insulin: Whipple’s triad • Gastrin • Vasoactive intestinal peptide etc.
Investigation • Biochemical markers • Radiological imaging
Investigation: biochemical markers • Specific markers depending on origin • Urinary 5-hydroxyindoleacetic acid (5-HIAA): main metabolite of serotonin • Gastrin • Insulin • Glucagon etc.
Investigation: biochemical markers Chromogranin A • Co-secreted by different neuroendocrine cell types • Correlates with tumour burden and stage • Established roles in literatures: • Diagnosis • Treatment response monitoring • Relapse detection
Chromogranin A • Relatively high sensitivity 53-85% Ben L. Endocrinol Metab Clin N Am 40 (2011) 111–134 • Non-specific • Elevated in non-NETs condition: • Non-neoplastic: chronic atrophic gastritis; renal failure; liver cirrhosis • Neoplastic: HCC; colon cancers • Drugs: proton pump inhibitors
Investigation: radiology • Computed tomography: • arterial enhancing lesions with washout in venous phase • Magnetic resonance imaging: • more sensitive for liver and bone marrow metastases
Endoscopic ultrasound • High sensitivity for tumours at esophagus, stomach, duodenum, and pancreas • Allows image-guided biopsy
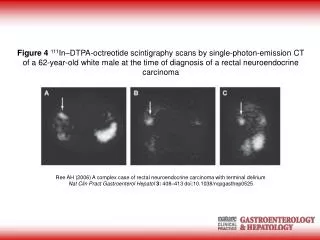
Octreoscan • Somatostatin (SST) receptor scintigraphy • Principle: 80-90% of NETs express SST receptors • Inflammatory lesions and some non-NET malignancies may give false positive results
Positron Emission Tomography • Ga-68 DOTATOC: high binding affinity for SST receptors • 18-FDG: identifies clinically aggressive lesions with high metabolism
PET: pros and cons • Better spatial and contrast resolution giving higher sensitivity • Specific radioisotopes not widely available • Hasn’t been fully validated with strong evidence yet
Principle of imaging for GEPNETs • CT or MRI combining with functional imaging to obtain maximal information • Currently Octreoscan is still the gold standard for radionuclide imaging • Will likely be replaced by PET scan with specific radioisotopes
Management • Surgical • Non-surgical
Management • Surgery remains the only curative treatment • Curative surgery should always be considered if feasible
Palliative surgery in metastatic disease: • Debulking • Resection of primary tumour Proven benefit for local and hormonal symptom control
Surgery • Surgical plan dictated by: • Tumour’s site of origin • Degree of tumour burden • General health or debility of the patient
Operative consideration • Perioperative somatostatin analogs • Prevents excessive hormone release during manipulation • Particularly important for intestinal carcinoids
Somatostatin (SST) analogs • First line medication • Acts through SST receptors on NETs • Inhibition of cellular proliferation and hormonal release • Available for clinical use: octreotide and lanreotide
SST analogs • Reduction in tumour size: <10% • Stabilization of tumour: 40-60% • Biochemical response: 50-70% • Symptomatic response: 70-90% Evidence of tumour response AND improvement of quality of life are well established
SST analogs • No conclusive evidence for survival benefit with use of SST analogs
Alpha-Interferon (IFN) • Induces apoptosis • Antiproliferative and anti-angiogenic effects • Evidence suggested usage in low-proliferating NETs only
Radionuclide therapy:Radiolabelled SST analogs • SST analogs, IFN, chemotherapies, and external irradiation all have poor response in advanced or rapidly progressing GEPNETs
Radiolabelled SST analogs • GEPNETs: high level of SSTR expression and good vascularization • Studied radionuclide agents: • 90Y-DOTA-octreotide • 111In-pentetreotide • 177Lu-DOTA-Tyr-octreotide
90Y-DOTA-octreotide • Encouraging short and intermediate term results: • 23-28% objective response rate • 63-70% symptomatic response rate • Longer progression free survival for pancreatic NETs Waldherr et al. J Nucl Med. 2002; 32:133-140 Paganelli G et al. Biopolymers 2008; 66: 393-398 • No long term result available yet
Cytotoxic chemotherapy • Sensitivity of NETs correlates with primary tumour location and tumour grade • low grade carcinoid tumours typically resistant • First line therapy only for metastatic/ unresectable pancreatic NETs • combination of streptozotocin and 5-fluorouracil (5-FU) • Some evidence for use in high grade ileal NETs
Targeted therapy • Mammalian target of rapamycin (mTOR): serine kinase regulating cell growth and proliferation • mTOR inhibitor: everolimus • Two recently completed phase III studies (RADIANT 2 and RADIANT 3) demonstrated statistically significant improvement in progression-free survival (PFS) in metastatic carcinoid tumours
Targeted therapy • NETs are highly vascular and frequently overexpress VEGF ligand and receptor • Bevacizumab and sunitinib: VEGF inhibitors • Phase II studies for both agents are promising • Multinational phase III study ongoing
Liver-directed therapies • Liver is the predominant site of metastases for GEPNETs • Metastatic liver disease gives more carcinoid syndrome • Treatment options: • Liver resection/ ablation • Hepatic artery embolization
Liver resection/ ablation • Advocated if more than 90% of tumours can be successfully resected or ablated • Symptom palliation and survival prolongation well reported
Hepatic artery embolization • Diffuse unresectable liver metastases • Rationale: tumours derived majority of their blood supply from arterial circulation • Bilobar metastases: staged lobar embolization at 4-6 weeks interval
Conclusion • GEPNETs represent a complex and heterogenous tumour entity with rising incidence and prevalence • Diagnostic and therapeutic challenges due to its relative rarity
Conclusion • Diagnostic and treatment options for GEPNETs are expanding • Controversies exist for choice and sequencing of treatments requiring relevant expertise input • Multidisciplinary approach warranted for best outcome for patients
Investigation: biochemical markers Urinary 5-hydroxyindoleacetic acid (5-HIAA) • Main metabolite of serotonin • helps diagnosing carcinoid syndrome • Not applicable for non-functional tumours
Operative consideration (2) • Role of prophylactic cholecystectomy • Rationale: somatostatin analogs treatment leads to development of gallstones • However most of these stones are asymptomatic • No conclusive evidence to recommend prophylactic cholecystectomy
Side effects of SST analogs • Usually mild: flatulence; abdominal pain; diarrhea in less than 10% patients • Choledolithiasis: in 20-40% patients with long term SST analogs; acute symptoms rare
SST analogs + IFN • Combination therapy as upfront treatment in therapy-naïve patients is not well established • Evidence for additive effect of tumour response: • sequential use of the two drugs; and, • combination after progression with single agent • No proven survival benefit
Side effect profile (Radiolabelled SST analogs) • Toxic effects are mild in most patients • Nausea and vomiting being the commonest symptoms • Severe lymphopenia and renal toxicity have been reported Waldherr et al. J Nucl Med. 2002; 32:133-140 Paganelli G et al. Biopolymers 2002; 66: 393-398 De Jong M et al. Int J Cancer 2001 Jun 1; 92(5): 628-33 Ebrahim S et al. Cancer biotherapy and radiopharmaceuticals Vol 23, No. 3, 2008