Download
1 / 30
310 likes | 568 Views
The Foot & Toes. Athletic Injury Assessment Chapter 4 P. 87. Clinical Anatomy— p. 87. Muscles— Intrinsic Extrinsic Sections (fig. 4-2) Rearfoot Midfoot Forefoot. Rearfoot— p. 88. Calcaneus & Talus Features: Achilles Tendon Sustentaculum Tali

E N D
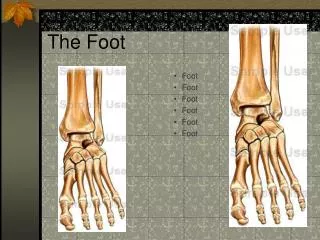
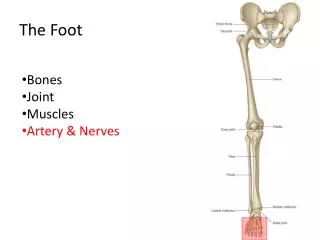
The Foot & Toes Athletic Injury Assessment Chapter 4 P. 87
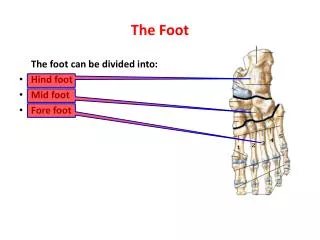
Clinical Anatomy—p. 87 • Muscles— • Intrinsic • Extrinsic • Sections (fig. 4-2) • Rearfoot • Midfoot • Forefoot
Rearfoot—p. 88 • Calcaneus & Talus • Features: • Achilles Tendon • Sustentaculum Tali • Subtalar joint (sup. calcaneus/ inf. Talus)
Midfoot—p. 88 • Navicular, cuboid, 3 cuneiform bones (Tarsals) • Shock absorbing section of the foot • Tibialis posterior inserts on navicular
Forefoot/Toes—p. 89 • 5 metatarsals, 14 phalanges • 50% of weight borne on the 1st and 5th toes • Each MT and Phalanx has a base, shaft, and head
Arches of the foot—p.91 • Arches: • Medial longitudinal • Lateral longitudinal • Transverse metatarsal • Dissipates ground reaction forces • More prominent in NWB
Medial Longitudinal Arch—p. 96 • Navicular is the keystone • Dysfunction at navicular (sprain) weakens the arch • Stability: • Spring ligament • Deltoid lig. • Plantar fascia • Dynamic stability of Ant. Tib., Post. Tib., and muscle • Fig. 4-6,p.96
Lateral Longitudinal Arch—p. 97 • Calcaneus, Cuboid, 5MT • Continuation of Med. Long. Arch • Rarely site of isolated injury
Transverse Metatarsal Arch—p. 97 • Tarsals and MT’s • Fig. 4-9,p. 98
Clinical Evaluation: HistoryP. 98-99 • Location of pain • Retrocalcaneal pain • Heel pain • Medial arch pain • Metatarsal pain • Great Toe pain • Onset of pain? • Acute vs. Chronic • Gradual/Insidious • Training changes • Shoes/orthotics
Clinical Evaluation: Observationp. 101-102 • Figure 4-11, p. 102 • Ambulatory aids? • Swelling/ecchymosis/ deformity? • Shoe wear patterns? • Callus formations? • Observe in WB and NWB • “Pump Bumps”—fig 4-16, p. 107 • Assess supination/ pronation • Assess arches
Plantar Warts Vs. Callus • Plantar Warts • Plantar aspect of foot • Usually in WB area of foot (callused area) • Often point tender • Well defined borders • Normal skin markings are masked • “stepping on a pebble” • Callus • WB/friction area • Not point tender superficially • Less defined borders • Normal swirl markings (whorls)
Pathological Toe Presentations—p. 105 • Box 4-2 • Ingrown nails • Subungual hematomas • Hammer toes • Morton’s toes • Hallux Valgus • Bunion/Bunionette
Clinical Evaluation: Palpation—p.108-112 • Assess Talar Neutral position (fig. 4-17, p. 107) • Divide foot into zones • Palpate structures for tenderness
Range of Motion Testing—p. 113 • Greatest with the Great Toe and least with 5th toe • AROM at MP joint assessed • Great Toe assessed independently • Assess rigidity of joints in toes and MT
Ligamentous Testing—p. 114 • Varus stress testing (LCL) • Valgus stress testing(MCL) • Box 4-6, p. 116 • Overpressure in PROM • Joint Glides • Intermetatarsal Glide • Box 4-7 • Tarsometarsal Glides • Box 4-8 • Midtarsal Glides • Box 4-9
Neurological Examination—p. 116 • Foot innervation: L4 & S2 • Nerve Compression: • Direct Trauma • Contusion • Entrapment • Indirect Trauma • Edema • Stretch
Arch Pathologies—p. 120Pes Planus • “Flat Feet” • Congenital, Biomechanical, or Traumatic onset • Navicular displaces medially • Look for accessory navicular (fig. 4-27, p. 120) • Assess in WB and NWB for supple pes planus (Box 4-10, p. 122)
Pes Planus • Treatment: • Orthotics • Strengthening: • Ant. Tibialis • Post. Tibialis • Toe flexors • Assess Navicular Drop • Box 4-11, p. 123 • (+) drop of >10 mm • Contributes to: • Eversion Sprains • MT stress fx • LBP • ACL sprains
Arch Pathologies—p. 121Pes Cavus • “High Arch” • High medial long. Arch • Calluses found PIP heads often • Increased load on arch
Pes Cavus—p. 121 • Contributes to : • MT, tibial, or fibular stress fx • Associated with scoliosis? • Treatment: • Orthotics to absorb added stress • Callus reduction/blister control • Proper fitting shoes • Surgical options: • Plantar fascia release
Plantar Fasciitis—p. 124 • Pain in longitudinal arch • Worsened by pes planus & pes cavus • Injury may congenital or traumatic • Often bilateral • Often found with tight HC • May accompany heel spurs • Treatment: • Identify cause! • Orthotics • Aggressive stretching program • Address biomechanics • Night splints for DF • Cortisone injections? • Surgical correction available
Heel Spur—p. 125 • Calcaneal exostosis (15% of population are asymptomatic) • Gradual onset with pain at heel strike aspect of gait • Signs & symptoms similar to plantar fasciitis (Table 4-7, p. 125) • May accompany plantar fasciitis • Tenderness @ toe flexor insertions • Treat as plantar fasciitis • Sx intervention may help
Tarsal Tunnel Syndrome—p. 126Table 4-8, p. 127 • Entrapment of the posterior tibial nerve • Fig. 4-30, p. 127 • Acute or gradual onset • Worsened by pronation and med. Arch problems (P. Planus) • Often confused with plantar fasciitis • Complaints: -diffuse medial foot/leg pain, burning, numbness that worsens with activity/stretching -(+) Tinel sign • Treatment:orthotics and possible surgery
Metatarsal Fractures—p. 128Table 4-9, p. 130 • Result from compression, tensile, rotation, or crushing forces • Higher incidence in diabetics • Signs/Symptoms; • False joint • Obvious deformity possible • Pain in WB • “March Fractures” • Jones Fractures
Intermetatarsal Neuromas-p.129Table 4-9, p. 130 • Entrapment of nerve between MT heads • Between 3rd & 4th=Morton’s Neuroma • Pain with WB • Pain worse when in shoes • Numbness/paresthesia • Mimics stress fx • Nodule may be palpable at site of numbness
Hallux Rigidus—p. 131 • Progressive degeneration of 1st MP joint • Results in limited motion 2º fusing of the joint • Biomechanics worsen and degeneration increases
Hallux Rigidus—p. 131 • Palpable exostosis at MP joint • Limited ext. of 1st MP • Altered gait • Pain at MP with activity • Confirmed via x-ray
First MP Joint Sprains—p. 132 • “Turf Toe” • Hyperextension OR hyperflexion of 1st MP • Varus/Valgus • Painful with palpation • Localized edema • Limited AROM • Treatment: • Identify cause • Taping • Orthotics/firm sole