Download
1 / 30
300 likes | 405 Views
Non-striated muscle II. Hospital Volunteer Wanna-bes.

E N D
Hospital Volunteer Wanna-bes • Pullman Regional Hospital is now accepting volunteer applications for the spring semester. Applications are due no later than Wednesday, January 18, 2012. Students may find more information about volunteering and the application requirements at https://www.pullmanregional.org/wsu-student-volunteers. • With best regards, • Kim Cook
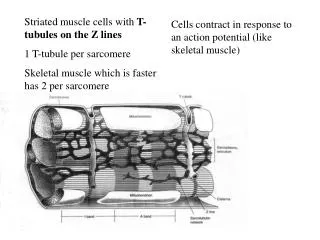
Excitation-contraction coupling: Two sources of Ca++ for smooth muscle contraction • Extracellular: through L Ca++ channels • Intracellular: from cell-surface associated SR (calciosomes)
Two routes for excitation-contraction coupling • Route 1: Electromechanical: depolarization opens L Ca++ channels in sarcolemma; L channels open nearby calciosome release channels (ryanodine receptors) by Ca++-induced Ca++ release. Each L channel thus ignites a calcium spark.
Route 2: Pharmacomechanical: transmitter or hormone sends 2nd message to calciosomes (and possibly also to L channels) to induce Ca++ release/entry.
Ach stimulates (constricts) airway GI tract pupillary constrictors Ach inhibits (dilates) specialized (genital) vasculature myocardium Contraction or relaxation? It all depends on the 2nd message(s) the muscarinic receptor is coupled to
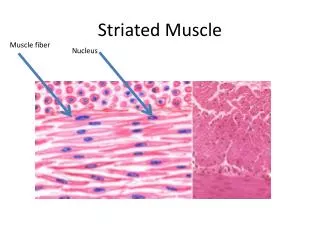
Ach causes action potentials and contraction in toad gastric smooth muscle. The voltage is measured by the microelectrode. The letters above the trace indicate the timing of the video frames.
A DAG-IP3 2nd Message: contraction of smooth muscle by acetylcholine Step 1. Acetylcholine released by the parasympathetic branch of the autonomic nervous system, binds to the muscarinic receptor for acetylcholine of intestinal smooth muscle. Step 2: The combination of neurotransmitter and receptor activates G protein
Step 3: G protein activates membrane-bound Phospholipase C Step 4: Phospholipase C converts some phosphatidylinositol bisphosphate (a membrane phospholipid) into inositol trisphosphate (IP3) and diacylglycerol. (DAG)
Phospholipase C splits off the “tails” of the phospholipid as DAG, and adds a phosphate to the “head” to form IP3
Step 5: Now the story splits into two directions. Direction 1: Still in the plasma membrame - DAG remains in the membrane. It activates Protein Kinase C, which has to translocate into the membrane to become active. Once PKC is active, it can phosphorylate many proteins, both membrane bound and free.
Direction 2: In the cytoplasm - IP3 diffuses through the cytoplasm. It binds to a receptor on the endoplasmic reticulum, a storage site for Ca++, causing Ca++ release.
Final Effects: Through PKC, DAG activates membrane channels that result in depolarization, with a change in the basic electrical rhythm. Through IP3, Ca++ is released from internal stores and the force of contraction is increased.
How the muscarinic receptor excites GI smooth muscle The electromechanical route: 1. Muscarinic receptor coupled to IP3-DAG 2nd message. 2. DAG activates protein kinase C 3. PKC inhibits rest K+ channels, causing depolarization. 4. Depolarization activates L channels 5. L channels activate Ca++ release from calciosomes.
The pharmacomechanical route 1. Muscarinic receptor coupled to IP3-DAG 2nd message. 2. IP3 activates release of Ca++ from calciosomes
A classic experiment with intestinal smooth muscle • Remove length of intestine from animal • Tie one end to rigid support • Attach other end to force transducer • Submerge muscle in heated, oxygenated saline.
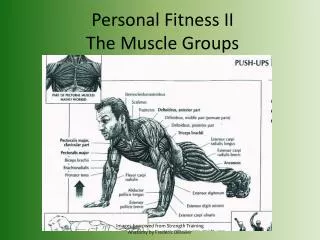
The anatomy of the intestinal muscularis Myenteric plexus (yellow) Submucosal plexus (orange) Longitudinal muscle outer layer) –dominated by electromechanical route Circular muscle (inner layer) – dominated by pharmacomechanical route Interstitial cells of Cajal (green)
The preparation is spontaneously active; acetylcholine both shortens the muscle and increases the magnitude of the oscillations. Isotonic length 1 min Upward displacements of the trace correspond to decreases in length
Ca++-free saline can be used to dissect the electromechanical and pharmacomechanical mechanisms Isotonic length Spontaneous contractions are eliminated in Ca++-free saline, which abolishes the electromechanical route; addition of acetylcholine can still elicit episodes of contraction by the pharmacomechanical route, but these diminish in magnitude with each subsequent addition (why?).
Epinephrine abolishes spontaneous activity and causes the muscle to go to a longer length Isotonic length
How the beta2 receptor turns off contraction in GI smooth muscle • 1. 2 receptor is coupled to cAMP 2nd message. • 2. cAMP activates Protein kinase A • 3. PKA phosphorylates MLCK • 4. Phosphorylated MLCK cannot be activated by calmodulin-Ca++
Norepinephrine Beta adrenergic receptor cAMP PKA MLCK-P (inactive)
Excitation Ach Serotonin Peptides (motilin) Inhibition catecholamines Vasoactive Intestinal Peptide/nitric oxide Dopamine Endogenous opiates There are many endogenous transmitter substances in the gut
NOS = nitric oxide synthase G-cyclase = guanylyl cyclase G-kinase =cGMP dependent protein kinase L-nmma and L-name are inhibitors of NOS O2 and HbO2 get rid of NO by oxidizing it
Let’s get to the point – some anatomy In the flaccid penis (and clitoris), cavernous arteries are constricted and the small amount of volume flow into the sinuses easily drains into the veins. Erection is the result of dilation of the cavernous arteries and trabecular smooth muscle. As the sinuses fill with blood under arterial pressure, they compress the vessels in the venular plexus, making outflow more difficult.
How sympathetic input causes you to lose it, or not even get it Smooth muscle contraction = vascular sinus deflation
The understanding of the nature and origin of EDRF as NO led rapidly to the development of drugs that act on this system. For example, Viagra and its congeners act by inhibiting a form of cGMP phosphodiesterase that is specific to genital vasculature. The drugs are not perfectly specific, so side effects include hypotension and a mild impairment of color vision (remember that phototransduction also involves a cGMP 2nd messenger, so you can see why effects on vision might occur). Patients who take nitroglycerine for their angina should not also take Viagra – why not?