Download
1 / 1
10 likes | 108 Views
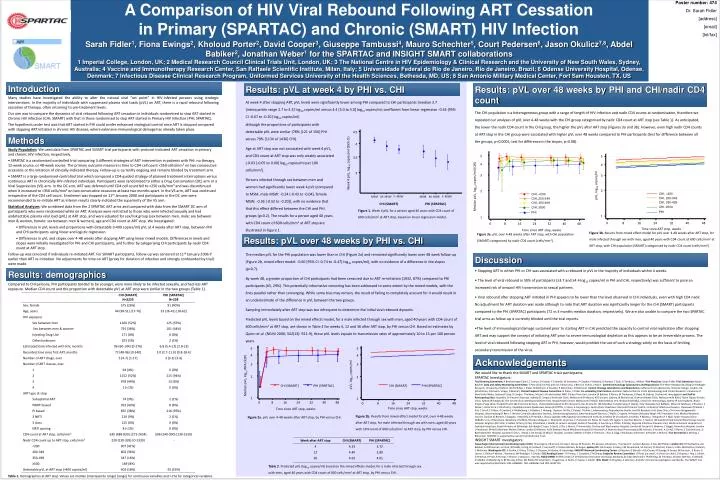
A Comparison of HIV Viral Rebound Following ART Cessation in Primary (SPARTAC) and Chronic (SMART) HIV Infection. Poster number: 474 Dr. Sarah Fidler [address] [email] [tel/fax]. 4.5. 4. 3.5. Week 4 pVL, log 10 copies/ml (95% CI). 3. CHI, <200. CHI, <200. CHI, 350-499. CHI, 200-349.

E N D
A Comparison of HIV Viral Rebound Following ART Cessation in Primary (SPARTAC) and Chronic (SMART) HIV Infection Poster number: 474 Dr. Sarah Fidler [address] [email] [tel/fax] 4.5 4 3.5 Week 4 pVL, log10 copies/ml (95% CI) 3 CHI, <200 CHI, <200 CHI, 350-499 CHI, 200-349 F: MSW F: MSW MSM M: MSW MSM M: MSW CHI, 200-349 CHI, ≥500 CHI, 350-499 CHI (SMART) PHI (SPARTAC) PHI CHI, ≥500 PHI 5 5 4 4 3 3 pVL, log10 copies/ml Median pVL, log10 RNA (IQR) 2 2 CHI (SMART) PHI (SPARTAC) CHI (SMART) PHI (SPARTAC) 1 1 0 8 16 24 32 40 48 0 8 16 24 32 40 48 Time since ART stop, weeks Time since ART stop, weeks Sarah Fidler1, Fiona Ewings2, Kholoud Porter2, David Cooper3, Giuseppe Tambussi4, Mauro Schechter5, Court Pedersen6, Jason Okulicz7,8, Abdel Babiker2, Jonathan Weber1 for the SPARTAC and INSIGHT SMART collaborations 1 Imperial College, London, UK; 2 Medical Research Council Clinical Trials Unit, London, UK; 3 The National Centre in HIV Epidemiology & Clinical Research and the University of New South Wales, Sydney, Australia; 4 Vaccine and Immunotherapy Research Center, San Raffaele Scientific Institute, Milan, Italy; 5 Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil; 6 Odense University Hospital, Odense, Denmark; 7 Infectious Disease Clinical Research Program, Uniformed Services University of the Health Sciences, Bethesda, MD, US; 8 San Antonio Military Medical Center, Fort Sam Houston, TX, US Introduction Results: pVL over 48 weeks by PHI and CHI/nadir CD4 count Results: pVL at week 4 by PHI vs. CHI Many studies have investigated the ability to alter the natural viral “set point” in HIV-infected persons using strategic interventions. In the majority of individuals with suppressed plasma viral loads (pVL) on ART, there is a rapid rebound following cessation of therapy, often returning to pre-treatment levels. Our aim was to compare the dynamics of viral rebound following ART cessation in individuals randomised to stop ART started in Chronic HIV Infection (CHI; SMART) with that in those randomised to stop ART started in Primary HIV Infection (PHI; SPARTAC). The hypothesis under test was that ART started in PHI could confer enhanced virological control once ART is stopped compared with stopping ART initiated in chronic HIV disease, where extensive immunological damage has already taken place. At week 4 after stopping ART, pVL levels were significantly lower among PHI compared to CHI participants (median 3.7 [interquartile range 2.7 to 4.3] log10 copies/ml versus 4.4 [3.0 to 5.0] log10 copies/ml; coefficient from linear regression -0.44 [95% CI -0.67 to -0.20] log10 copies/ml) The CHI population is a heterogeneous group with a range of length of HIV infection and nadir CD4 counts at randomisation, therefore we repeated our analyses of pVL over 4-48 weeks with the CHI group categorised by nadir CD4 count at ART stop (see Table 1). As anticipated, the lower the nadir CD4 count in the CHI group, the higher the pVL after ART stop (Figures 3a and 3b). However, even high nadir CD4 counts at ART stop in the CHI group were associated with higher pVL over 48 weeks compared to PHI participants (test for difference between all the groups, p<0.0001; test for difference in the slopes, p=0.08). although the proportions of participants with detectable pVL were similar (78% [121 of 156] PHI versus 79% [1134 of 1436] CHI). Age at ART stop was not associated with week 4 pVL, and CD4 count at ART stop was only weakly associated (-0.03 [-0.05 to 0.00] log10 copies/ml per 100 cells/mm3). Persons infected through sex between men and women had significantly lower week 4 pVL (compared to MSM, male MSW: -0.24 [-0.43 to -0.04], female MSW: -0.36 [-0.52 to -0.20]), with no evidence that that this effect differed between the CHI and PHI groups (p=0.2). The results for a person aged 40 years with CD4 count of 600 cells/mm3 at ART stop are illustrated in Figure 1. Methods • Study Population: We used data from SPARTAC and SMART trial participants with protocol-indicated ART cessation in primary and chronic HIV infection, respectively. • SPARTAC is a randomised-controlled trial comparing 3 different strategies of ART intervention in patients with PHI: no therapy, 12-week course, or 48-week course. The primary outcome measure is time to CD4 cell count <350 cells/mm³ on two consecutive occasions or the initiation of clinically-indicated therapy. Follow-up is currently ongoing and remains blinded by treatment arm. • SMART is a large randomised-controlled trial which compared a CD4-guided strategy of planned treatment interruptions versus continuous ART in chronically HIV-infected individuals. Participants were randomised to either a Drug Conservation (DC) arm or a Viral Suppression (VS) arm. In the DC arm, ART was deferred until CD4 cell count fell to <250 cells/mm³ and was discontinued when it increased to >350 cells/mm³ on two consecutive occasions at least two months apart. In the VS arm, ART was continued irrespective of the CD4 cell count. Enrolment was stopped on 11th January 2006 and participants in the DC arm were recommended to re-initiate ART as interim results clearly indicated the superiority of the VS arm. • Statistical Analyses: We combined data from the 2 SPARTAC ART arms and compared with data from the SMART DC arm of participants who were randomised while on ART. Analyses were restricted to those who were infected sexually and had undetectable plasma viral load (pVL) at ART stop, and were adjusted for sex/risk group (sex between men, male: sex between men & women, female: sex between men & women), age and CD4 count at ART stop. We investigated: • Differences in pVL levels and proportions with detectable (>400 copies/ml) pVL at 4 weeks after ART stop, between PHI and CHI participants using linear and logistic regression. • Differences in pVL and slopes over 4-48 weeks after stopping ART using linear mixed models. Differences in levels and slopes were initially investigated for PHI and CHI participants, and further by categorising CHI participants by nadir CD4 count at ART stop. • Follow-up was censored if individuals re-initiated ART. For SMART participants, follow-up was censored at 11th January 2006 if earlier than ART re-initiation. No adjustments for time on ART (proxy for duration of infection and strongly confounded by trial) were made. 5 5 4 4 3 3 pVL, log10 copies/ml Median pVL, log10 copies/ml (IQR) 2 2 Figure 1. Week 4 pVL for a person aged 40 years with CD4 count of 600 cells/mm3 at ART stop, based on linear regression model. 1 1 0 8 16 24 32 40 48 0 8 16 24 32 40 48 Time since ART stop, weeks Time since ART stop, weeks Figure 3b. Results from mixed effect model for pVL over 4-48 weeks after ART stop, for male infected through sex with men, aged 40 years with CD4 count of 600 cells/mm3 at ART stop, with CHI population (SMART) categorised by nadir CD4 count (cells/mm3). Figure 3a. pVL over 4-48 weeks after ART stop, with CHI population (SMART) categorised by nadir CD4 count (cells/mm3). Results: pVL over 48 weeks by PHI vs. CHI The median pVL for the PHI population was lower than in CHI (Figure 2a) and remained significantly lower over 48 week follow-up (Figure 2b, mixed effect model: -0.60 [95% CI -0.74 to -0.47] log10 copies/ml), with no evidence of a difference in the slopes (p=0.7). By week 48, a greater proportion of CHI participants had been censored due to ART re-initiation (1932, 87%) compared to PHI participants (65, 29%). This potentially informative censoring has been addressed to some extent by the mixed models, with the lines parallel rather than converging. While some bias may remain, the result of failing to completely account for it would result in an underestimate of the difference in pVL between the two groups. Sampling immediately after ART stop was too infrequent to determine the initial viral rebound dynamic. Predicted pVL levels based on the mixed effects model, for a male infected through sex with men, aged 40 years with CD4 count of 600 cells/mm3 at ART stop, are shown in Table 2 for weeks 4, 12 and 36 after ART stop, by PHI versus CHI. Based on estimates by Quinn et al. (NEJM 2000; 342(13): 921-9), these pVL levels equate to transmission rates of approximately 10 to 15 per 100 person years. Discussion • Stopping ART in either PHI or CHI was associated with a rebound in pVL in the majority of individuals within 4 weeks. • The level of viral rebound in 50% of participants (≥3.7 and ≥4.4 log10 copies/ml in PHI and CHI, respectively) was sufficient to pose an increased risk of onward HIV transmission to sexual partners. • Viral rebound after stopping ART initiated in PHI appears to be lower than the level observed in CHI individuals, even with high CD4 nadir. No adjustment for ART duration was made although to note that ART duration was significantly longer for the CHI (SMART) participants compared to the PHI (SPARTAC) participants (72 vs 3 months median duration, respectively). We are also unable to compare the two SPARTAC trial arms as follow-up is currently blinded until the trial reports. • The level of immunological damage sustained prior to starting ART in CHI predicted the capacity to control viral replication after stopping ART and may support the concept of initiating ART prior to severe immunological depletion as this appears to be an irreversible process. The level of viral rebound following stopping ART in PHI, however, would prohibit the use of such a strategy solely on the basis of limiting secondary transmission of the virus. Results: demographics Compared to CHI persons, PHI participants tended to be younger, were more likely to be infected sexually, and had less ART exposure. Median CD4 count and the proportion with detectable pVL at ART stop were similar in the two groups (Table 1). Acknowledgements We would like to thank the SMART and SPARTAC trials participants. SPARTAC Investigators: Trial Steering Committee: A Breckenridge (Chair), C Conlon, D Cooper, F Conradie, M Schechter, P Claydon, P Kaleebu, G Ramjee, F Ssali, G Tambussi, J Weber. Trial Physician: Sarah Fidler. Trial Statistician: Abdel Babiker. Data and Safety Monitoring Committee: T Peto (Chair) A McLaren (in memoriam), V Beral, G Chêne, J Hakim. Central Immunology Laboratories and Repositories: The Peter Medawar Building for Pathogen Research, University of Oxford, UK (R Phillips, J Frater, N Robinson, P Goulder, P Klenerman, N Robinson). Central Virology Laboratories and Repositories: Jefferiss Trust Laboratories, Imperial College, London, UK (M McClure, O Erlwien, S Kaye, D Bonsall). Clinical Endpoint Review Committee: N Paton, S Fidler. Co-ordinating Trial Centres: Australia: National Centre in HIV Epidemiology and Clinical Research, University of New South Wales, Sydney (P Grey, D Cooper, T Kelleher, M Law). UK and Ireland: MRC Clinical Trials Unit, London (A Babiker, K Porter, M Thomason, K Boyd, M Gabriel, D Johnson). Investigators and Staff at Participating Sites: Australia: St Vincent’s Hospital, Sydney (D Cooper), Northside Clinic, Melbourne (R Moore), 407 Doctors, Sydney, (R McFarlane), Prahran Market Clinic, Melbourne (N Roth), Taylor Square Private Clinic, Sydney (R Finlayson), The Centre Clinic, Melbourne (B Kiem Tee), Sexual Health Centre, Melbourne (T Read), AIDS Medical Unit, Brisbane (M Kelly), Centre for Immunology, Sydney (P Cunningham). Brazil: Projeto Praça Onze, Hospital Escola São Francisco de Assis, Universidade federal do Rio de Janeiro, Rio de Janeiro. (M Schechter, R Zajdenverg, P, Gama). Italy: Ospedale San Raffaele, Milan (G Tambussi, V Rusconi, S Nossa, L Della Torre, C Ronchetti,), Ospedale Lazzaro Spallanzani, Roma (G D’Offizi, C Vlassi, A Corpolongo). South Africa: Capetown: Desmond Tutu HIV Centre, Institute of Infectious Diseases, Capetown (R Wood, J Pitt, C Orrell, F Cilliers, R Croxford, K Middelkoop, L G Bekker, C Heiberg, J Aploon, N Killa, E Fielder, T Buhler ) Johannesburg: Reproductive Health and HIV Research Unit, Bara Clinic, Chris Hani Baragwanath Hospital, Johannesburg (H Rees, F Venter) Contract Laboratory Services, Johannesburg Hospital, Johannesburg (W Stevens, C Wallis, C Ingram, M Majam) Kwazulu-Natal: HIV Prevention Unit, Medical Research Council, Durban (G Ramjee, S Gappoo, J Moodley, A Premrajh, L Zhao,) Uganda: MRC/Uganda Virus Research Institute, Entebbe (H Grosskurth, A Kamali, P Kaleebu, J Mugisha, H F Njaj). Spain: Hospital Clinic-IDIBAPS. Univ. of Barcelona. Barcelona (J M Miro, M López-Dieguez, C. Manzardo, JA Arnaiz, T. Pumarola, M. Plana, M. Tuset, MC Ligero, V. Sanchez-Merino, T. Gallart, JM Gatell) UK and Ireland: Royal Sussex County Hospital, Brighton (M Fisher, K Hobbs, N Perry, D Pao, D Maitland, L Heald), St James’s Hospital, Dublin (F Mulcahy, G Courtney, S O’Dea, D Reidy), Regional Infectious Diseases Unit, Western General Hospital and Genitourinary Dept, Royal Infirmary of Edinburgh, Edinburgh (C Leen, G Scott, L Ellis, S Morris, P Simmonds), Chelsea and Westminster Hospital, London (B Gazzard, D Hawkins, C Higgs), Homerton Hospital, London (J Anderson, M Kall), Mortimer Market Centre, London (I Williams, N De Esteban) North Middlesex Hospital (J Ainsworth, A Waters), Royal Free Hospital (M Johnson, S Kinloch, A Carroll, P Byrne, Z Cuthbertson), St Bartholomew’s Hospital, London (C Orkin, J Hand, C De Souza), St Mary’s Hospital, London (J Weber, S Fidler, E Thomson, J Fox, K Legg, S Mullaney, A Winston, N Poulter, S Wilson). Trial Secretariat: S Keeling, J Bohannon. SPARTAC is supported by a grant from Wellcome Trust. INSIGHT SMART Investigators: Copenhagen International Coordinating Center (ICC): JD Lundgren, KB Jensen, DC Gey, L Borup, M Pearson, PO Jansson, BG Jensen, J Tverland, H. Juncker-Benzon, Z Fox, AN Phillips. London ICC: JH Darbyshire, AG Babiker, AJ Palfreeman, SL Fleck, W Dodds, E King, B Cordwell, F van Hooff, Y Collaco-Moraes, BJ Angus. Sydney ICC: DA Cooper, S Emery, FM Drummond, SA Connor, CS Satchell, S Gunn, S Oka, MA Delfino, K Merlin, C McGinley. Washington ICC: F Gordin, E Finley, D Dietz, C Chesson, M Vjecha, B Standridge. INSIGHT Network Coordinating Center: JD Neaton, G Bartsch, A DuChene, M George, B Grund, M Harrison, E Krum, G Larson, C Miller, R Nelson, J Neuhaus, MP Roediger, T Schultz. ECG Reading Center: R Prineas, C Campbell, Z-M Zhang. Endpoint Review Committee: G Perez (co-chair), A Lifson (co-chair), D Duprez, J Hoy, C Lahart, D Perlman, R Price, R Prineas, F Rhame, J Sampson, J Worley. NIAID DSMB: M Rein (chair), R DerSimonian (executive secretary), BA Brody, ES Daar, NN Dubler, TR Fleming, DJ Freeman, JP Kahn, KM Kim, G Medoff, JF Modlin, R Moellering Jr, BE Murray, B Pick, ML Robb, DO Scharfstein, J Sugarman, A Tsiatis, C Tuazon, L Zoloth. NIH, NIAID: K Klingman, S Lehrman. And 667 clinical site investigators worldwide. The SMART trial was supported by NIH Grants U01-AI068641, U01-AI046362 and U01-AI042170. Figure 2b. Results from mixed effect model for pVL over 4-48 weeks after ART stop, for male infected through sex with men, aged 40 years with CD4 count of 600 cells/mm3 at ART stop, by PHI versus CHI. Figure 2a. pVL over 4-48 weeks after ART stop, by PHI versus CHI. Table 2. Predicted pVL (log10 copies/ml) based on the mixed effects model, for a male infected through sex with men, aged 40 years with CD4 count of 600 cells/mm3 at ART stop, by PHI versus CHI. Table 1. Demographics at ART stop. Values are median (interquartile range) [range] for continuous variables and n (%) for categorical variables.






