Download

1 / 36
390 likes | 482 Views
Best Practices at IU Health. Marc Goldman, MBA, MSW System Director, Learning & Service Excellence, IU Health Arnett. Session Purpose. Encourage experimentation with new ways to improve how we fulfill our Promise of Assurance Share some emerging Best Practices from within our own system

E N D
Best Practices at IU Health Marc Goldman, MBA, MSW System Director, Learning & Service Excellence, IU Health Arnett
Session Purpose • Encourage experimentation with new ways to improve how we fulfill our Promise of Assurance • Share some emerging Best Practices from within our own system • Dedicate time to begin action planning your next steps
It Pays to Imitate… • Good imitators actively seek ideas worth copying. • Imitation is not the “easy” path. • Finding best practices to imitate is everyone’s job. • Excerpts from: • It Pays to Imitate: A Closer Look at the Dynamics of Best Practices, by QuintStuder
…The Dynamics of Best Practices • Diagnose what the best practice really is. • Create a best practice transfer manual. • Outline the outcomes you want and the processes that will take you there. • Consider what questions to anticipate & the “pushback” that might come from others • Spell out and sequence the steps necessary for implementing the best practice. • Don’t get too hung up on “best.” • Excerpts from: • It Pays to Imitate: A Closer Look at the Dynamics of Best Practices, by QuintStuder
Our Agenda • Three Emerging Best/Better Practices • Today’s Panel of LTP Internal Coaches: • Linda House • Lorraine Brown • Joshua Georgen & Monica Shane • Small Group Dialogue & Action Planning • Q & A with our Panel
Call Light Response Project Linda House, RN, BSN, MBA Director of Clinical Operations Medical Division & LTP Internal Coach IU Health Methodist Hospital
Project Goal • Create a standardized process for answering call lights for all MH Inpatient Medical/Surgical and OB units based on patient centeredness • Increase staff awareness of call light priority over routine tasks
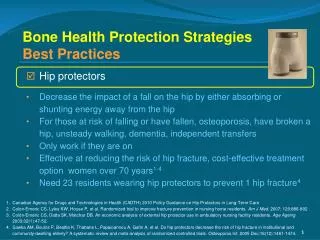
Expected Outcomes • Improve the patient experience through: • Decreasing response time of call lights • Improving the patients’ perception of the response time to call lights • Reducing injury to patients by a more prompt response time to call lights (i.e. falls from patients needing to go to the bathroom)
Current State Project Onset • Average response time for MH – 3 minutes • Several individual units had average response times hovering around 4 minutes • Large variation in practices from unit to unit – no unit following same process for answering lights • Structure in place to push daily reports to managers measuring CL response times
Structure • Met with all managers to review current practices • Conducted Literature Search – (answer CL within 1 minute; respond within 5 minutes) • Formed focus group (Mgrs, Staff RNs, USs) to gain input on standardization of process and creation of flow chart • Proposal submitted to Director group with approval • Training materials created • Process rolled out to managers – Dec 2011 • Training of staff – January/February 2012 • Observation, validation, and competency completion
Training • Mandatory two hour training sessions for all US • US Training Content • Why change current practice – Is Pt. satisfaction really important? - Introduction to HCAHPS/VBP - Storytelling • Customer Service – Outcomes vs. Pt. Perception • Communication Makeovers • Face-to-Face Service Excellence • Telephone Service Excellence • New Process • Role Play • RN & Support Staff training conducted by Mgrs
Together We’re Stronger by Reducing the Number of Patients Who Fell
Next Steps • Ongoing Validation on Nursing Units • Feedback/Coaching of Staff • Embed in US Orientation • Continue Monitoring Data
Questions and Answers • Contact Information: Linda House RN,BSN,MBA Director of Medical Division IU Health Methodist Hospital 317-962-1122 lhouse@iuhealth.org
Rounding with patients transferred to IUH Arnett from IUH White Lorraine Brown, MSN, RN Administrative Director for Inpatient Services & LTP Internal Coach IUH Arnett
Rounding on transferred patients The Problem: • IUH White does not receive feedback from patient transferred to IUH Arnett. The Practice: • Intentionally round on patients transferred from White to get feedback on: • their hospital experience at White • their understanding of the need for transfer to another facility.
Process steps We had a patient admitted today from IUH White ED. • Patient: • PCP: • Diagnosis: • Unit: • Admitting physician: • Email sent by Arnett patient placement. • IUH White recipient: • Administrator IUH Arnett recipients: • Case Management Director • Inpatient Services Director • Switchboard/Patient Placement Director • Trauma Services Coordinator • Unit Manager receiving the patient • Unit Manager rounds with the patient • Feedback is provided back to IUH White Administrator who forwards to Senior & Unit leaders • Any gaps in communication or care the patient/family might have perceived while a patient at IUH White are addressed
Outcomes • Implementing this process has allowed us to follow up on some process issues that we would have never known without the intentional rounding. • Examples include: transport issues and issues with explaining the need for transfer to the patient. • Feedback from the patient is almost always positive. • This allows the individuals involved to know that their efforts made a difference to the patient. • The purpose of the process is all about SERVICE to the patient.
Lessons Learned • Email initially did not include the unit manager. Result: Process breakdown. • By adding the manager, a step in the process was removed and the feedback could be provided in a more direct, timely manner. • On weekends/holidays, the Associate Administrators are made aware of the transfer and complete the follow up process. • Awareness of IUH commitment to service extends beyond our walls due to the number of times we transfer patients from other areas.
Questions and Answers • Contact Information: Lorraine Brown, MSN, RN Administrative Director for Inpatient Services IU Health Arnett lbrown26@iuhealth.org
Visit Guide / Question Card Joshua Georgen Team Lead, Service Excellence & LTP Internal Coach IU Health Physicians Monica Shane Director, Patient Access & LTP Internal Coach IU Health Arnett
Visit Guide / Question Card • Tool that helps ensure we meet our patient’s needs prior to leaving the exam room • “During your most recent visit, did you have any health questions or concerns that you did not discuss with this provider?” • Given to patients during check-in/registration • Patients write down questions/concerns they want to discuss with the provider during their visit • Patients also have a place to mark action items they need (e.g. RX refill, return to work/school form, etc.) • Provider reviews prior to entering the exam room
Outcomes • Reduced patient calls post-visit • Reduced number of times patients stopped at the front desk after their visits to obtain information they forgot to discuss • Increased patient satisfaction scores 6-mo post implementation (University Hospital AOC)
Lessons Learned • Partner with physician/provider sponsors to ensure understanding and support • Engage Front Desk and Clinical Staff in identifying key words to use when explaining the form • Keep extra forms in exam rooms for clinical staff to hand out if the patient misplaced or discarded it • Unit leaders began reviewing completed forms daily to promote accountability & recognition • Hardwiring requires long-term focus
Lessons Learned, cont. • The visit guide should be accompanied by • eliciting the full spectrum of patient concerns • positively setting the agenda with the patient.1 • The visit guide can be detrimental if filled out by patient and then not used properly (or at all) by provider (e.g. dissatisfied patients, increased visit time, etc). 1Stein, T., Krupat, E., & Frankel, R., PhD. 2011. Talking with Patients: using the Four Habits Model. The Permanente Medical Group, Physician Education and Development.
Next Steps • IUH Arnett is now spreading 3-Question Card process to all its outpatient physician office practices. • Form content has been integrated into the Pre-Visit Summary (PVS) starting 4-24-13
Questions and Answers • Contact Information: Joshua Georgen Team Lead, Service Excellence & LTP Internal Coach IU Health Physicians jgeorgen@iuhealth.org Monica Shane Director, Patient Access & LTP Internal Coach IU Health Arnett mshane3@iuhealth.org
Small group Dialogue & Action Planning • Divide into small groups of about 3-5 • Share if you are interested in adopting one of these practices, or if you have other ideas in mind • Use the “lean-based” action planner – Continue to explore one or more ideas until time is called • Be ready to share: • Ideas your small group discovered • Realizations, important points, “aha” moments • Questions for the panel