Download
1 / 80
830 likes | 1.05k Views
Klinefelter Syndrome. Kristin Clemens PGY 5 Endocrine Rounds January 30, 2013. Case. 20 year old male Presents to new family doctor for physical. No known medical conditions Inguinal hernia repair No medications, no significant family history Puberty at age 13, tall compared peers

E N D
Klinefelter Syndrome Kristin Clemens PGY 5 Endocrine Rounds January 30, 2013
Case 20 year old male Presents to new family doctor for physical
No known medical conditions Inguinal hernia repair No medications, no significant family history Puberty at age 13, tall compared peers Development seemed to slow Learning disability, behavioural problems Didn’t finish high school Living at home
Tall, long legs, BMI 30 kg/m2 Normal cardiac, respiratory and abdominal exams Scant facial and chest hair Bilaterally small testicles – 4mL Klinefelter syndrome?
Objectives To learn about the origin of Klinefelter syndrome and understand it’s genetics To review its many clinical manifestations and associated medical co morbidities To learn how to optimally manage patients with the condition
Klinefelter Syndrome Most common sex chromosome aneuploidy seen in clinical practice 1 in 500 live male births Increased maternal age ?Association with paternal age
First described by Klinefelter in 1942 Reports of 9 men with gynecomastia, sparse facial and body hair, small testes and an inability to produce sperm
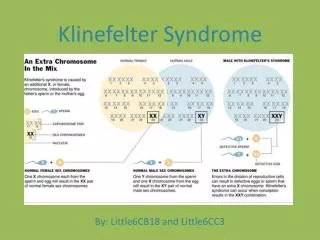
Genetics Extra X chromosome first documented in 1959 Classically 47 XXY – 89% 48 XXXY among other variants Non-disjunction – abnormal partitioning of chromosomes
Non-disjunction:Meiosis Abnormal partitioning of chromosomes during meiosis such that the resultant haploid gametes have too many or too few chromosomes
Meiotic non-disjunction Meiosis I Meiosis II genetics.thetech.org
53% result from 1st paternal meiotic non disjunction 34% from 1st maternal meiotic non disjunction 9% 2nd meiotic division
Non disjunction:Mitosis Mosaic 47 XXY Mitotic non disjunction within the zygote 10% of cases Variable phenotype Typically less severe Depends on the specific tissues in which an extra X chromosome is present If normal karyotype in the testis may have intact spermatogenesis and fertility
Pathogenesis:Extra X Chromosome(s) Genes of X chromosome play an important role in the sex development in males and females at the level of the gonad More than 100 X chromosome genes are expressed in the testes
Genes on extra X chromosome: Testicular failure - progressive loss of germ cells, seminiferous tubule hyalinization and fibrosis Low testosterone Progressive hypogonadism
Furthermore… Androgen receptor gene on X chromosome Variable CAG repeats on exon 1 Length of the highly polymorphic CAG repeat inversely related to AR activity Short lengths more stable with more marked effect of androgens Longer lengths less stable- androgen insensitivity
In Klinefelter’s, at least 2 X chromosomes Shortest CAG repeat is preferentially inactivated – non-random X chromosome inactivation Less effective androgen receptor Further contributes to the phenotype
Infancy and Childhood Micropenis Small testes Normal surge of testosterone over 1-6 months Early gonadal dysfunction and decreased fetal testosterone in utero
Hypospadias Cryptochordism Hypotonia Cleft palate Inguinal hernia
Hypertelorism Elbow dysplasia Clinodactyly High arched palate Journal of Pediatrics
Delayed developmental progress Delayed gross and fine motor skills Adjustment disorders Deficits in language and executive function Dyslexia ADHD Emotional difficulties
Pre-puberty may see disproportionate lower component compared with upper Tall stature for familial size Unfused growth plates secondary to androgen deficiency Narrow shoulders, broad hips
Puberty Normal onset of puberty with rise in testosterone, LH, FSH until about 13 to 14 years or Tanner stage 3 puberty Slow progression or arrest of pubertal changes Impaired Leydig cell reserve and low testosterone levels Testicles fail to increase in size and become firm due to a progressive loss of germ cells and seminiferous tubule hyalinization and fibrosis Incomplete virilization with AR instability
Gynecomastia • 15% of estrogen secreted by testes as estradiol or estrone • Rest from peripheral conversion from testosterone • 95% from the testicles • Adipose tissue has P450 aromatase activity important for transforming androstenedione into estrone • Conversion increases with age and obesity
Breast tissue development Balance between estrogen and testosterone Estrogen stimulates the growth and differentiation of breast epithelium Androgens inhibit the growth and development of breast tissue
Why gynecomastia in Klinefelter’s? High circulating LH levels stimulate aromatase activity in Leydig cells leading to higher levels of estradiol relative to testosterone Low testosterone Alteration in estrogen to androgen ratio from high estrogen or low androgen concentrations Breast tissue enlargement
Adulthood • Signs/symptoms of hypogonadism • Infertility • Gonadal failure and loss of germ cells from tubule hyalinization and fibrosis of seminiferous tubules
Osteoporosis Decreased bone mass in 20-50% of patients and osteoporosis in up to 15%
Low testosterone? Testosterone aromatized to estrogen which decreases bone resorption Also effects osteoblasts directly through the androgen receptor Promotes periosteal bone formation and reduces bone resorption through adult life Need testosterone to achieve peak bone mass
Ferlin et al 2011 Cross-sectional cohort study 112 treatment naïve KS XXY and 50 aged matched controls 43% of KS patients had low bone mass No significant relationship between testosterone, bone markers (calcium, phosphate, albumin, PTH, 25 hydroxyvitamin D) and bone mass CAG repeats not different in those with normal and low bone mass
Likely multifactorial Other contributors may include abnormal androgen receptor, X chromosome inactivation, increase fat mass and reduced muscle mass, low vitamin D levels Low insulin like factor 3 levels produced by Leydig cells
Lung pathology Bronchitis Bronchiectasis Unknown pathophysiology
Malignancies • Germ cell tumours • Mediastinal tumours in 8% (50x expected rate) • Relative risk of 67 in cancer registries • Need to consider in those with known Klinefelter’s and precocious puberty • Non-Hodgkins lymphoma • Acute leukemia
Breast cancer 20 fold increase in breast cancer Denmark cohort of 832 KS found that 3.7 to 7.5% had BC Brinton et al studied 4.5 million men in US Veterans Affairs and noted 3518 cases of male breast cancer with 642 in Klinefelters RR 16.83 (6.81-41.62) Alteration in endogenous hormone ratios, genetic predisposition, presence of gynecomastia
Autoimmune conditions SLE RA
Cardiovascular anomalies Mitral valve prolapse Aortic valvular disease Berry aneurysms Varicose vein Ulcers
Danish registry Thromobophlebitis and venous thrombosis HR 5.29 (3.29-8.5) PE HR 3.6 (1.92-6.74) CAD HR 1.71 (1.28-2.29) Abnormalities in plasminogen 1, clotting factors, obesity
Endocrine Graves disease Thyroiditis Dyslipidemia DMII
DMII Jiang-Feng et al Retrospective longitudinal study of 39 men with Klinefelter’s and 40 with idiopathic hypogonadotropic hypogonadism Prevalence of diabetes in KS group was 20.5% and in the IHH group 5% Testosterone effect on insulin sensitivity IM testosterone (approximately 4 years) to keep total levels <10 nmol/L
?Testosterone effect doesn’t explain whole story Extra copy of X chromosome leads to decreased insulin sensitivity or insulin resistance Autoimmune disease? Metabolic syndrome, increased weight Increased truncal fat and waist measurements during childhood, adolescence and adulthood
Variable presentation Genetics – the more X chromosomes, the more severe CAG length
CAG lengths Those with short CAG repeat lengths found to have more stable relationships, higher educational levels, greater responses to testosterone treatment If long CAG and reduced AR activity, have longer arms and legs, smaller testes, lower BMD, greater degree of gynecomastia