Download
1 / 115
1.4k likes | 1.59k Views
Leukemia. Liu Hui MD Dep.Hematology,General Hospital,TMU. Fig 3 A child actor. Fig 1 Marie Curie. Fig 2 Song Qingling. General introduction. Definition Classification Etiology Incidence and prevalence. Abridged general view of normal hemapoiesis Hemapoietic stem cells(HSC)

E N D
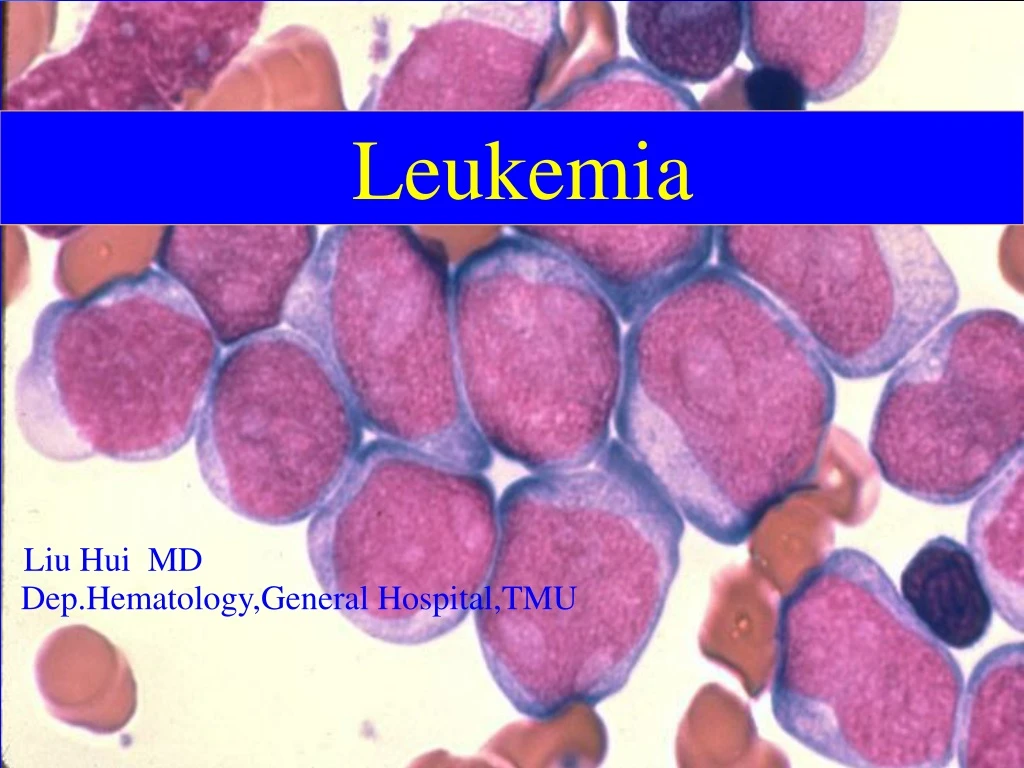
Leukemia Liu Hui MD Dep.Hematology,General Hospital,TMU xie Yi,Hua Shan Hospital
Fig 3 A child actor Fig 1 Marie Curie Fig 2 Song Qingling
Definition • Classification • Etiology • Incidence and prevalence
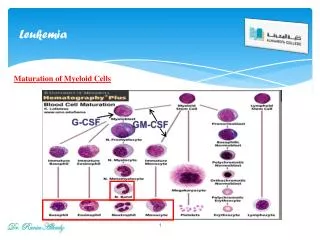
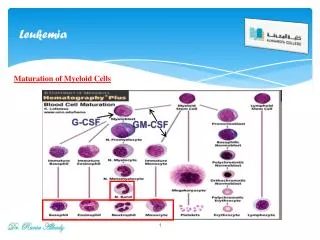
Abridged general view of normal hemapoiesisHemapoietic stem cells(HSC) progenitor cells pronormoblast monoblast myeloblast lymphoblast megakaroblasterythrocytes monocytes granulocytes lymphocytes platelets
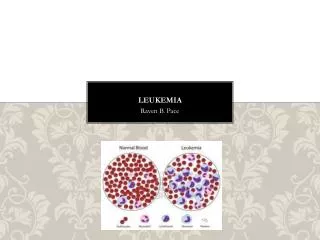
Definition • A heterogeneous group of neoplasms arising from the malignant transformation of hematopoietic cells. • Leukemia cells proliferate primarily in the bone marrow and lymphoid tissues where they interfere with normal hematopoiesis and immunity • They emigrate into the peripheral blood and infiltrate other tissues
Classification • Acute • Acute myeloblastic leukemia • Acute lymphoblastic leukemia • ( have a rapid clinical course) • Chronic • Chronic myelocytic leukemia • Chronic lymphocytic leukemia • (have a more prolonged natural history)
Etiology • The cause is not known in most patients • 1. Virus • 2. Environmental factors • 3. Genetic factors
Etiology • 1.Virus : a unique human retrovirus • 1) Human T-cell leukemiavirus I • (HTLV-I ): adult T-cell leukemia • (ATL) • 2) Human T-cell leukemiavirus II • (HTLV-II) : chronic T-cell leukemia( CTL)
Etiology • 2. Environmental factors: radiation 1、atom bomb (长 崎)1Km 1.5km 2km × 100×22 × 2.6 2、high dose X radiation、32P therapy
Etiology • 2. Environmental factors:Chemicals • --benzene • --treatment with alkylating agents and other chemotherapeutic drugs lead to an increased incidence of AML
Etiology • 3. Genetic factors • Identical twins of AL • Congenital disorders
Incidence and prevalence Incidence: 2.76 / 100,000 people / year in China Sex predilection: somewhat higher in men than in women Peak age incidence: AML: at all ages CML: adults ALL : children and a part of the elderly CLL : in the elderly
Mechanism Radiation, chemicals, virus, genetics & other blood disorders Chromosome translocation Fusion gene formation Fusion protein(enzyme …… ) Malignant biologic behaviors Malignant blood disorders
Acute leukemia • Acute myeloblastic leukemia • Acute lymphoblastic leukemia
Clinical features • Anemia • Bleeding • Infection • Organ and tissue infiltration
Clinical features • 1.Anemia : the first sign including pallor , fatigue, weakness, palpitations and dyspnea on exertion
Clinical features • 2. Bleeding : related to thrombocytopenia • petechiae and easy bruisability are common; • hemorrhage becomes increasing common when the PLT count is less than 20,000/ul. • Spontaneous bleeding invovling the central nervous system,lungs,or other viscera may also occur.
Clinical features • 3.Infection: a frequent complication of AML • common sites: skin, gingiva,lungs,and urinary tract. • Septicemia often occurs without an apparent source. • Fever is present in many patients at the time of diagnosis.
Clinical features • 4.Organ and tissue infiltration • Hepatomegaly, splenomegaly, lymphadenopathy, sternal tenderness • Special infiltration area • Chloromas:skin ,orbit (granulocytic sarcoma) • Painless enlargement of testicle( ALL) • CNS involvement, paraplegia(ALL,M4,M5) • gingivitis(M4,M5)
Organ and tissue infiltration Urogenital system lungs Cardiovascular system Oral and gastrointestinal bone、joint Leukemic cells skin Central nervous system eyes
leukostasis Caused by high level of circulating blasts(>80,000 to 100,000) acute respiratory distress,CNS bleeding and thromboses,tumor lysis syndrome leukapheresis
Classification • Seven subtypes • M1 • M2 • M3 • M4 • M5 • M6 • M7
Morphologic subtypes of AML • M1: • AML without maturation , 20% of AML • Morphology : few if any azurophilic granules in cytoplasm • Reactivity with special stains: • Peroxidase(POX)/sudan black: +/– • Nonspecific esterase: +/– • Periodic acid schiff (PAS): –
Morphologic subtypes of AML • M2: • AML with maturation , 30% of AML Morphology : blasts with promyelocytic granules, auer rods may be persent • Reactivity with special stains: • POX/sudan black: +++ • Nonspecific esterase: +/– • PAS: +
Morphologic subtypes of AML • M3: • Acute promyelocytic leukemia , 5% of AML Morphology : Hypergranular promyelocytes often with multiple auer rods per cell • Reactivity with special stains: • POX/sudan black: +++ • Nonspecific esterase: + • PAS: +
Morphologic subtypes of AML • M4: • Acute myelomonocytic leukemia , 30% of AML • Morphology :both myeloblastic and monoblastic leukemic cells in blood and marrow • Reactivity with special stains: • POX/sudan black: ++ • Nonspecific esterase: +++ • PAS: ++/+
Morphologic subtypes of AML • M5: • Acute monocytic leukemia , 10% of AML • Morphology :Leukemic cells are large and often bizarre; nuclear cytoplasmic ratio 1:1 or less. Cytoplasm contains fine granules. Auer rods are rare, nucleus is often convoluted and contain one to four large nucleoli • Reactivity with special stains: • POX/sudan black: +/– • Nonspecific esterase: +++ • PAS: ++/+
Morphologic subtypes of AML • M6: • Acute erythroleukemia , 5% of AML • Morphology :erythroblasts are in abundance initially in marrow and often in blood • Reactivity with special stains: • POX/sudan black: – • Nonspecific esterase: – • PAS: ++
Morphologic subtypes of AML • M7: • Acute megakaryocytic leukemia , 5% of AML • Morphology : Large and small megakaryoblasts with high nucleus/cytoplasm ratio, pale agranular cytoplasm . undifferentiated blasts react with antiplatelet antibodies and contain platelet peroxidase • Reactivity with special stains: • POX/sudan black: – • Nonspecific esterase: +/ – • PAS: +
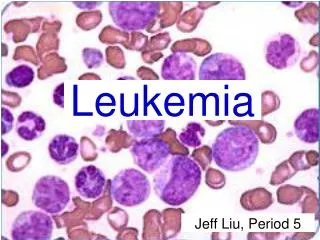
Diagnosis of AML • Blood --Severe thrombocytopenia,normocytic anemia,circulating peripheral blasts. • Bone marrow --myeloblasts 20%-100% - in non erythrocytic cells(NEC) of bone marrow smear
MICM TYPING DIAGNOSIS • MICM • Morphology • Immunology • Cytogenetics • Molecular
Morphology • Myeloblasts are distinguished from lymphoblasts by any of two pathognomonic features: • 1. histochemical stains: AML:POX+, NSE+ ALL:PAS+++ • 2. Auer rods in the cells
IMMUNO-PHENOTYPING mab M1 M2 M3 M4 M5 M6 M7 CD13 + + + + + - - CD33 + + + + + - - CD14 - ± - + + - - CD41 - - - - - - + GlycoA - - - - - + - Lectoferrin - + - + - - - CD19 CD7 HLA-DR CD2 MPO T - + - + - B + - + - -
Chromosome translocation M1 +8,-5,-7 inv(3) M2 t(8;21)(q22;q22), t(6;9) M3 t(15;17)(q22;q21), M4 inv(16) M5 t(4;11), t(8;16) M6 M7 ALL t(9;22) t(8;14)
Fusion gene molecular • AML1/ETO • PML/RAR • CBF/MYH11 • MLL abnormalites • BCR/ABL
Differential Diagnosis • Myelodysplastic syndrome (MDS) refractory anemia or pancytopenia, BM: dysplasia, blasts<20% • Leukemoid reaction mature leukocytes proliferative would play a main role, NAP↑, if progenitor increase, only shortly on time • CML: mature progenitors ↑ Eosinophil↑、Basophil↑, NAP=0, ph'(+),bcr-abl(+) • Infectious mononucleosis,agranulocytopenia There is no blasts in bone marrow
Therapy • Supportive care • Chemotherapy • Hemapoietic stem cell transplantation
Supportive care • Antibiotic therapy • The use of Growth factors that stimulate granulopoiesis • Component transfusion therapy
Antibiotic therapy • Pancytopenia after treatment is a sign of effective drug action • The patient usually becomes febrile(>38oC),often with associated rigors, and cultures of stool, urine, blood, throat, and , if available, sputum should be obtained • Antibiotic therapy should be started immediately after cultures are obtained