Download
1 / 21
210 likes | 215 Views
Explore the value and methodological strengths and weaknesses of real-world evidence (RWE) in the context of medical research. Understand how RWE complements randomized controlled trials (RCTs), its data sources and limitations, and the differences in terminology. Discover how RWE can contribute to the translation of RCT findings into high-quality evidence for routine clinical practice.

E N D
Real-world evidence Value, methodological strengths and weaknesses
Context What is RWE? RWE, real-world evidence. 1. Food and Drug Administration. RWE. https://www.fda.gov/ScienceResearch/SpecialTopics/RealWorldEvidence/default.htm (Accessed July 2019).
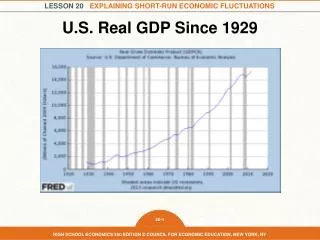
Context Growing recognition of RWE within medicine • There has been increasing recognition of the potential value of RWE in recent years as reflected by its increasing presence within the medical literature1 Year *Search algorithm: “real-world” OR “real world” OR “real-life” Or “real life”. RWE, real-world evidence.1. US National Library of Medicine National Institutes of Health. PubMed. https://www.ncbi.nlm.nih.gov/pubmed/ (Accessed April 2019).
Context RWE complements RCT evidence Real-world studies: enable evaluation of: RCTs: required for regulatory approval • RWE can: • Confirm whether RCT results are observed in everyday clinical practice1 • Provide complementary insights from more varied settings1 • Help to translate RCT findings into high-quality evidence that can guide routine clinical practice1 *e.g. different age, race, comorbidities, co-medications, adherence. RCT, randomised controlled trial; RWE, real-world evidence.1. Nallamothu BK, et al. Circulation 2008;118(12):1294–303.
Data RWE data Real-world data source example: claims data
Data RWE data Real-world data source example: EHRs EHRs: electronic health records.
Data RWE data Examples of real-world data sources and the oncology-related questions they can address *Cancer-specific (i.e. not linked to wider health records). Generally: Evaluable; Unevaluable; Feasible to infer, or subject to data collection.
Data RWE data Real-world data limitations AE, adverse events; RCT, randomised controlled trial. 1. SouthworthMR, et al. N Engl J Med 2013;368(14):1272; 2. Larsen TB, et al. J Am CollCardiol 2013;61(22):2264–73.
Methods RCTs vs real-world studies: characteristics RCT, randomised controlled trial. 1. KhozinS, et al. J Natl Cancer Inst 2017;109(11); 2. Roche N, et al. Ann Am ThoracSoc 2014;11(Suppl. 2):S99–S104; 3. NallamothuBK, et al. Circulation 2008;118(12):1294–303.
Methods RCTs vs real-world studies: characteristics1–4 *The approval of an extended indication of palbociclib (for the treatment of men with HR+, HER2- metastatic breast cancer) was based predominantly on RWE4 †Through patient selection and optimised standards of care. HCP, healthcare professional; RCT, randomised controlled trial; RWE, real-world evidence. 1. Khozin S, et al. J Natl Cancer Inst 2017;109(11); 2. Roche N, et al. Ann Am ThoracSoc 2014;11(Suppl. 2):S99–S104; 3. Nallamothu BK, et al. Circulation 2008;118(12):1294–303; 4. Wong GWK, et al. Ann Am ThoracSoc 2014;11(Suppl. 2):S85–91; 4. Pfizer. Press Release. https://www.pfizer.com/news/press-release/press-release-detail/u_s_fda_approves_ibrance_palbociclib_for_the_treatment_of_men_with_hr_her2_metastatic_breast_cancer (Accessed July 2019)
Methods RWE/RCT terminology differences PFS, progression-free survival; RCT, randomised controlled trial; RWE, real-world evidence; TTP, time to progression. Commonly used terminology often differs for real-world studies and RCTs:
Methods Describing study designs in real-world terms The framework links various types of studies based on: population characteristicsand ecology of care The typical position of common study designs are illustrated, but can be moved in any direction depending on the specifics of its study design 1. Roche N, et al. Lancet RespirMed 2013;1(10):e29–30.
Methods PRECIS wheel: describing study designs using ten explanatory pragmatic axes1 Explanatory studies: Tests a causal research hypothesis: ‘Does a treatment work under ideal conditions?’ Pragmatic studies: Helps to choose between care options: ‘Does a treatment work under usual conditions?’ RCT, randomised controlled trial. 1. Thorpe KE, et al. J ClinEpidemiol 2009;62(5):464–75.
Results Interpreting RCT findings and RWE Real-world studies often make use of proxy endpoints if specific variables are not routinely available RCT endpoints and real-world outcomes can differ; methodological review is required before comparing their findings: *Time from study enrolment for single-arm trials; **TTF may discriminate between discontinuations due to adverse events and discontinuations for other reasons.AE, adverse event; PD, progressive disease; PFS, progression-free survival; RCT, randomised controlled trial; RECIST, Response Evaluation Criteria in Solid Tumors; RWE, real-world evidence; TTF, time to treatment failure; TTP, time to progression.
Results Endpoints – PFS, TTP, TTF: RCT scenario1 Conceptual scenario: Prolongation of median progression free survival by treatment beyond progression outweighs the effect of treatment discontinuation for other reasons. AE, adverse events; mPFS, median progression-free survival; RCT, randomised controlled trial; TTF, time to treatment failure; TTP, time to progression.
Results Endpoints – PFS, TTP, TTF: RCT scenario2 Conceptual scenario: the effect of treatment discontinuation for other reasons has more effect than prolongation of mPFS by treating beyond RECIST progression. AE, adverse events; mPFS, median progression-free survival; RCT, randomised controlled trial; RECIST, Response Evaluation Criteria in Solid Tumors;TTF, time to treatment failure; TTP, time to progression.
Results Outcomes – TTP, ToT (TTF/TTD): RW scenario Conceptual scenario: Routine care patients treated as long as clinician deems beneficial. A greater number of events (e.g. PD, withdrawal, discontinuation due tolerability) contribute to ToT (TTF) analyses, making it shorter than TTP. AE, adverse events; PD, progressive disease; RECIST, Response Evaluation Criteria in Solid Tumors; RW, real-world; ToT, time on treatment; TTF, time to treatment failure; TTP, time to progression.
Results Interpreting RWE: comparing vs RCT results *Through patient selection and optimised standards of care. OS, overall survival; RCT, randomised controlled trial; RWE, real-world evidence. 1. Karim S, Booth CM. J ClinOncol 2019:37(13):1047–50.
Results Side-by-side comparison: real-world effectiveness vs RCT efficacy Results: Author conclusions: • Baseline cohort: in real-world patients eligible for RCTs, real-world OS benefits were: • Similar to those observed in RCTs based on OS endpoints • 16% less than RCTs based on surrogate endpoints (PFS, TTP) • Full cohort: in non-selected real-world populations, treatment benefit was predicted to be even less than in the baseline, RCT-eligible real-world cohort *Not reported in Ladawalla et al; included for illustrative purposes to exemplify the direction of the observed differences. EHR, electronic health record; HR, hazard ratio; MHR, mortality hazard ratio; OS, overall survival; PFS, progression-free survival; RCT, randomised controlled trial; SEERS, Surveillance and Epidemiology End Results; SHR, surrogate hazard ratio; TTP, time to progression. 1. Lakdawalla DN, et al. Value in Health 2017;20(7):866–75 Objective: • Measure the relationship between RCT efficacy and real-world effectiveness for oncology treatments, in: • Selected real-world patients who meet routine RCT eligibility criteria (Baseline cohort) • All real-world patients with evaluable records (Full cohort) Methods: • RCT data: abstracted from 21 Phase III oncology RCTs reporting OS or PFS or TTP • RW data: EHRs – SEERs Medicare data • Primary outcome: real-world OS, estimated as MHR • Cox proportional hazard regression model used to calibrate difference between RW MHR and: • RCT MHR • RCT PPS/TTP SHR
Results Pragmatic real-world endpoints in NSCLC studies: considerations Analysis of time-to-treatment discontinuation of targeted therapy, immunotherapy, and chemotherapy in clinical trials of patients with non-small-cell lung cancer1 Results (cont’d): Author conclusions: • mTTD exceeds mPFS for oncogene-targeted subgroups due to treatment beyond RECIST progression. The ability to treat beyond progression may reflect real-world treatment tolerability • With ICI therapy, mPFS (4.2 months) was slightly longer than mTTD (3.5 months), with cases of both early and late TTD. This may reflect some: cases of early termination due to immune-mediated AEs; some instances of durable treaetment benefit, and others of treatment beyond conventional progression • Further research is needed to validate TTD as a measure for pragmatic RCTs Methods: • 18 metastatic NSCLC RCTs: • Initiated after 2007 • Submitted to the FDA • Involved 8947 patients • Compared TTD to PFS and OS • TTD: defined as date of randomisation to date of discontinuation or death Results: • Overall: TTD was more closely associated with PFS (r=0.87, 95% CI 0.86–0.87) than with OS (r=0.68, 95% CI 0.67–0.69) • Oncogene-targeted subgroups: mTTDs exceeded mPFS: • EGFR+: 13.4 months vs 11.4 months, respectively • ALK+: 14.1 months vs 11.3 months, respectively AE, adverse event; ALK, anaplastic lymphoma kinase;ChT, chemotherapy; EGFR, epidermal growth factor receptor; FDA, US Food and Drug Administration; ICI, immune checkpoint inhibitor; maint., maintenance; mPFS, median PFS; mTTD, median TTD; NSCLC, non-small cell lung cancer; OS, overall survival; PFS, progression-free survival; RCT, randomised controlled trial; RECIST, Response Evaluation Criteria in Solid Tumors; TKI, tyrosine kinase inhibitor; TTD, time to discontinuation. 1. Blumenthal GM, et al. Ann Oncol 2019;30(5):830–8.
RWE Summary EMR, electronic medical records; RCT, randomised controlled trial; RWE, real-world evidence.1. Wong GWK, et al. Ann Am ThoracSoc 2014;11(Suppl. 2):S85–91; 2. Nallamothu BK, et al. Circulation 2008;118(12):1294–303; 3. Roche N, et al. Ann Am ThoracSoc 2014;11(Suppl. 2):S99–S104; 4. Karim S, Booth CM. J ClinOncol 2019:37(13):1047–50; 5. Lakdawalla DN, et al. Value Health 2017;20(7):866–75. • Background: • Real-world studies complement RCTs – they provide evidence from everyday patient populations managed in routine care settings, including those with characteristics that would preclude their participation in RCTs1–3 • Real-world data sources: • There is a wider range of real-world data sources available; each has specific strengths and limitations • Real-world data source examples include: electronic medical record databases (primary care ± secondary care ± pharmacy ± other linked data); insurance claims databases; patient access schemes; registries • Real-world studies vs RCTs:1,3 • Conducted for different purposes, e.g. drug registration (RCTs) vs long-term surveillance (real-world studies) • Differ according to how much their design reflects (i) real-world patients and (ii) real-world clinical management • Different strengths and weaknesses, e.g. real-world studies offer high external validity, but low internal validity • Real-world vs RCT findings: • Often evaluate different outcomes; real-world studies make use of proxy measures where specific variables are unavailable • RCTs may over-estimate treatment benefits through their selection of ‘ideal’ populations4 • Real-world studies and RCTs provide complementary evidence; a judicious approach combining evidence from both can provide a more complete view of the evidence base1–5