Download
1 / 32
330 likes | 371 Views
Oral symptoms of extraoral infections. Infections around oral cavity. Medical oral microbiology I – ZLLM0421p Week 14 Ondřej Zahradníček Based upon the slideshow of assoc. prof . Vladana Woznicová. Symptoms of microbial diseases directly in the oral cavity.

E N D
Oral symptoms of extraoral infections. Infections around oral cavity. Medical oral microbiology I – ZLLM0421p Week 14 OndřejZahradníček Based upon the slideshow of assoc. prof. Vladana Woznicová
Symptoms of microbial diseases directly in the oral cavity The oral cavity is a site that may witness the symptoms of various bacterial, viral, mycotic, eventually even parasitic infections They can be either local symptoms of an otherwise systemic infection, or eventually local symptoms of infections localised somewhere else. Rarely also local infection localised directly in the oral cavity
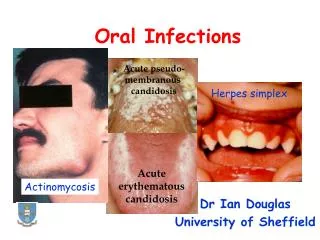
Infections in the oral cavity – survey Among common viral agents in the oral cavity, we have viruses of Herpesviridae, family, coxsackieviruses, papillomaviruses, measles and mumps viruses (Paramyxoviridae) Among bacterial agents, we have causative agens of syphilis, gonorrhoea, scarlet fever, diphtheria etc. As to mycotic agents, the most common one is Candida albicans, eventually other Candida sp. As for parasitic agents we sometimes find some protozoa (Endolimax gingivalis, Trichomonas tenax), rarely even tapeworm cysts
Infections caused by herpes simplex viruses (HSV1, HSV2) Primary infection of small children often inapparent, in older children small blisters on the tongue, palate and gum, itching or burning sensation, blisters develop, rupture and become ulcers. Gingiva is oedematous, painful and reddish Reactivation of infection has the form of classic herpes labialis. It occurs at different triggers. The virus is kept latent in sensoric ganglia Professional disease in stomatologists or dental hygienists is paronychium (herpes on fingers) Therapy uses aciclovir, diagnostics, if needed, is based on smears from lesions to the transport medium, antigen detection using immunofluorescence, eventually also serology
Herpes simplex primoinfection http://www.consultant360.com/article/punctate-oral-erosions-self-limited-%E2%80%9Csore%E2%80%9D%E2%80%94or-something-more-serious
Herpes simplex – herpes labialis http://www.vitalia.cz/katalog/nemoci/opar/
Infection of the chicken-pox and shigles virus(VZV, varicella-zoster virus) Before the typical skin rash in chickenpox (= primary infection here) develops, we can find lesions on the hard palate, pillars of the faces and uvula: small ulcers surrounded by an area of erythema, quickly rupture Oral manifestations of the secondary infection – herpes zoster (shingles) contains severe pain like in toothache, and enanthema* just on one side *Enanthema is something like exanthema (rash), but on mucosal membrane insted of skin.
Infection of the Epstein-Barr virus (EBV, virus of infectiousmononucleosis) Petechial haemorrhages at the junction of the hard and soft palates – Holzel´s sign are first signs. Later tonsillitis or tonsillofaryngitis occur (often resembling classic streptococcal one), submandibularlymfadenitis, sometimes even pseudomembranes occur in the throat Oedema of the complete Waldeyer lymphatic circle, sometimes even disablebreathing Particular case is EB virosis of HIV-positive people: not painful spots on margins of the tongue, so called hairy leucoplakia
Just as a review Waldeyer‘s lymphatic circle tonsillapharyngea tonsillaepalatinae tonsillalingualis tonsillaetubariae (Gerlachi) lymphatic tissue of lateral sides of pharynx lymphatic tissue of rear side of pharynx lymphatic tissue around beginning of pharynx
Infection of HHV-6 and measles virus Infection by human herpesvirus 6 (HHV-6) This is causative agent of exanthema subitum/roseola infantum (also 6thexantematic disease). Virus is present in the saliva, forms erythematous papules seen in soft palate and uvula (Nagayama´s spots) Infection by measles virus (morbillivirus) In prodromal state, Koplik‘s spots on bucalmucose against molars – little white spots surrounded by dark red margin *Prodromal period = period of starting, not yet specific signs
Enteroviral infections Enteroviruses are a group of viruses, that are transmitted by faecal-oral route, but the symptoms are mostly extraintestinal. Oral symptoms are common in so called coxsackieviruses and some newer enteroviruses Herpangina got its name after look of ulcers on mucosa of tonsils, palate and uvula – they resemble those in herpes. The ulcers are considerably small, diameter 1–2 mm, s greyish-white surface surrounded by red areolae. It is caused by coxsackieviruses A 2, A 4–6, A 8 Hand-foot-mouth disease – living red spots, in the mouth we can see oval greyish blisters with red limitation. Relatively common, but often not mentioned. Most frequent in South-East Asia Attention! Do not confuse this one with „foothand mouth disease“ of cattle, that is not transmissible to humans and is caused by completely different viruses
Herpangina http://zdravi.e15.cz/clanek/priloha-lekarske-listy/diferencialni-diagnostika-angin-a-nbsp-jejich-terapie-153319 Autor: Doc. MUDr. Pavel Smilek, PhD.
Hand-foot-mouth disease http://hardinmd.lib.uiowa.edu/dermnet/handfootmouth1.html
Changes in the oral cavity during HIV infection First indicators of HIV infections use to be mycotic opportune infections, e. g. oral candidosis (thrush) As to viruses (and eventual following cancers), we can see EB-virus specific damage – not painful whitish corrugated lesions on the tongue margins – hairy leukoplakia, Kaposi´s sarcoma, herpetic gingivostomatitis and oral papilloma Bacterial infection: gingivitis (linear marginal erythema/ ulcerous gingivitis), necrotizing stomatitis and necrotizing ulcerous parodontitis We can also see cervical lymphadenopathy, lymphomas
Mycotic infections in the mouth Oral candidiasis is mostly caused by Candida albicans. This yeas is an opportune patogen, infection usually occurs at some immunity problems. These immunity problems may be topic or systemic: skin lesions, teeth implants, malnutrition, diabetes mellitus, leukaemia, surgical operations, burnings, AIDS, immunosuppressive therapy, broad spectre antibiotic use Therapy is either local (clotrimazol, gentiane violet, iodine preparations), or, in more difficult cases, also systemic (fluconazole, itraconazoel, amphotericin B), autovaccines
Forms of mycotic infection I Pseudomembranouscandidiasis (thrush) is the most frequent one. We observe an erythematous mucous membrane with milk white pseudomembranes. It occurs in newborns (especially preterm newborns), older people, in immunocompromised is chronic, in HIV may spread into oesophagus Erythematous (atrophic) candidiasis in its acute form result after broad-spectrum antibiotic therapy, dysmicrobia of the oral cavity – mucous membrane. In the oral cavity, we can see erythematous areas, burning sensation.
Thrush http://detskechoroby.rodinka.sk/detske-choroby/hlava/usta-a-zuby/soor-zabka-mucnivka-mykoza-ust/ http://www.alternativni-medicina.eu/rozhovor-s-mudr-petrem-lukesem-dil-4-nizkotucne-vyrobky-cukr-coca-cola.html
Forms of mycotic infectionII Prosthetic stomatitis (chronic form of the previous) – frequently observed in elderly people wearing full dentures orthodontic appliances. The problems are mostly in palate and tongue. The mucosa in red and oedematous. Therapy: removal of dentures at night, cleaning and disinfection of dentures, carbohydrate diet Hyperplasticcandidiasis (candidaleukoplakia) – chronic, from small, palpable, whitish areas to large, dense plaques, hard and rough to touch, on the inside surface of cheeks. High risk of malignant transformation! Angular candidiasis is seen in one or both angles of the mouth, especially as a complication of prosthetic stomatitis, erythema and fissuring or vitamin B12 deficiency
Bacterial infections I: Syphilis Chancre (ulcus durum): a symptom of first stage of syphilis – may be present in the mouth of pharynx and considered to be e. g. tonsillitis Nevertheless, the most typical oral symptoms concern so called late inborn (congenital) syphilis: Hutchinson´s incisors upper central incisors: barrel-shaped, crescentic notch at the incisal edge Mulberry (moon) molars (Fournier‘s teeth) first molar teeth have a roughened dirty, yellow, hypoplasticocclusional surface, poorly developed cusps resembling the surface of mullbery.
Bacterial infections II Gonorrhoea, caused by gonococcus (Neisseria gonorrhoeae) may look as tonsillitis or pharyngitia. In can be also asymptomatically present in the pharynx or the oral cavity Scarlet fever is a disease caused by some strains of Streptococcus pyogenes; only strains forming erytrogenous toxin may do this. Exanthema on soft palate curves and uvula, coalescent, scarlet red enanthema, white coated tongue, rich red with markedly exserted papillae –raspberry tongue, enlarged+painfulsubmandibular lymph nodes. Skin rush – coalescent light red spots missing in perioral area Drug of choice is penicillin
Bacterial infections III Diphtheria is a serous disease caused by Corynebacterium diphtheriae. The disease is manifested as pseudomembranous tonsillitis/laryngitis (croup). A thick, adherent pseudomembrane is present on tonsils or pharynx, may involve nasal mucosa, the pharyngeal wall and the soft palate. Oedema involving the cervical lymph glands may occur in the anterior tissues of the neck – bullneck diphtheria.
TB and Leprosy in the oral cavity TB in the oral cavity is mostly characterised by ulcers, granulomas, fissures, diffuse inflammatory lesions Leprosy in the oral cavity may have different symptoms according to the form of infection: tuberculoid leprosy – paraesthesia of the face, lips, tongue, palate, cheeks or gingiva lepromatous leprosy – saliva is infectious, tooth loss, premaxillary bone resorption, saddle nose, intraoral nodules with tend to ulcerate
Viral salivary gland infections I Unlike the previous, they are not suppurative. Parotitis epidemica (mumps) – replication in salivary duct epithelial cells – pain on chewing, redning of the opening of the duct, enlargement of gland + decrease of saliva secretion Virus may be transmitted to the CNS ( serous meningitis, good luck – usually inapparent), or cause orchitis of adult males (painful+sterility), pancreatitis (increase of amylase level), eventually nephritis Diagnosis, if necessary is possible by means of electron microscopy, serology (IgM detection – immunofluorescence)
Viral salivary gland infections II Cytomegalovirus infection may be seen after reactivation of latent infection. In such case we often see sialoadenitis. This is more frequent in AIDS patients, people with immunosupression, or cytostatic therapy HIV (not frequently) may also have symptoms ofxerostomia and enlargement of the major salivary gland+ Sjögren´ssyndrom (dry keratoconjunctivitis and progressive polyarthritis)
Bacterial salivary gland infections Acute suppurativeparotitis (sialoadenitissuppurativa acuta) – very painful, absceding inflammation It is caused by alpha-haemolytic streptococci, S. aureus, haemophilus, eikenela, peptostreptococci After intraabdominal operation acute afteroperationparotitis, first serous, later absceding
Some more perioral infections Important is so called Ludwig‘s angina. It is a bilateral infection of sublingual and sumbadibular space with tendency to spreading. The most common causative agents are commensal bacteria originating in the oral cavity (mostly gram-negative anaerobic rods¨. These also are expected at microbiology examination. Suppurative inflammation of bone marrow of maxilla or mandibula is similar to that of any other osteomyelitis, but may be complicated by lost teeth. A slight difference against other osteomyelitis still exists: it is less frequently caused by staphylococci, more frequently the causative against come directly from the oral cavity. Actinomycosis of the face ant neck has also often origin in the oral cavity. In the soft tissues surrounding the oral cavity there is a focus of thick pus, sometimes open to the surface by a fistula.
Ludwig‘s angina http://perpetuum-lab.com.hr/forum/page/medicinski_eponimi/_/k-l/ludwigova-angina-r234
Thanks for attendance http://www.vitalia.cz/katalog/nemoci/ludwigova-angina/