Download
1 / 42
440 likes | 669 Views
HYPERSENSITIVITY. BY Dr Mahesh Mathur,MD , DCP (UK). PRE TEST. 1 . WHICH OF THE FOLLOWING CELLS ARE INVOLVED IN DELAYED TYPE HYPERSENSITIVITY A . LYMPHOCYTES B. EOSINOPHILS C. NEUTROPHILS D . MONOCYTESED 2. NOT AN EXAMPLE OF DELAY TYPE HYPERSENSITIVITY A.TISSUUE GRAFT REJECTION

E N D
HYPERSENSITIVITY BY Dr Mahesh Mathur,MD, DCP (UK)
PRE TEST 1. WHICH OF THE FOLLOWING CELLS ARE INVOLVED IN DELAYED TYPE HYPERSENSITIVITY A. LYMPHOCYTES B. EOSINOPHILS C. NEUTROPHILS D.MONOCYTESED 2. NOT AN EXAMPLE OF DELAY TYPE HYPERSENSITIVITY A.TISSUUE GRAFT REJECTION B.TUBERCULAR GRANULOMA C. ARTHUS RECATION D. CONTACT DERMATITIS 3. WHICH OF THE FOLLOWING STATEMENT IS NOT CORRECT A . BLOOD TRANSFUSION REACTION – TYPE II REACTION B. ALLOGRAFT REJECTION – TYPE IV REACTION C. SERUM SICKNESS – TYPE II REACTION 4. A GIRL DEVELOPED REDNESS & SWELLING OF EAR LOBULES AFTER WEARING SOME EARINGS THS IS A EXAMPLE OF WHICH TYPE OF HYPERSENSITIVITY A.CELL MEDIATED B..IMMUNE COMPLEX C.CYTOTOXIC D.IMMEDIATE TYPE
5. IN POS STREPTOCOCCAL GLOMERULONEPHRITIS THE TYPE OF HYPERSENSITIVITY INCLUDES • A. TYPE IV • B. TYPE III • C. TYPE II • D. TYPE I • 6. WHICH OF THE FOLLOWING IS THE TYPE I REACTION • A. SICK TEST • B. MOUNTOUX TEST • C. CASONI’S TEST • D. PATCH TEST • 7. WHICH OF THE FOLLOWING IS AN EXAMPLE OF IMMEDIATE HYPERSENSITIVITY • A. LEPROMINE TEST • B. SERUM SICKNESS • C. TUBERCULINE TEST • D. CASONI’S TEST
8. WHICH Ig IS RESPONSIBLE FOR TYPE I REACTION • A. IgM • B. IgA • C. IgG • D. IgE • 9. WHICH IS NOT A TYPE III REACTION • A.TUBERCULOSIS • B. RHUMATOID ARTHRITIS • C. SLE • D. ARTHUS REACTION • 10. ALL ARE TRUE ABOUT TYPE III REACTION EXCEPT • A. SERUM SICKNESS • B. ARTHUS REACTION • C. ANAPHYLAXIS • D. LUPUS NEPHRITIS
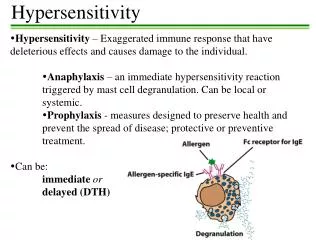
The term hypersensitivity describe immune responses which are damaging rather than helpful to the host. • Nearly 40 years ago Gell and Coombs proposed a classification scheme which defined 4 types of hypersensitivity reactions. • The first 3 are mediated by antibody, the fourth by T cells.
The Rapid ('Immediate') allergic reaction Type I • The symptoms produced by exposure of a sensitised person to antigen depend upon the site of contact. • Hayfever (allergic rhinitis), • eczema, • Asthma and urticaria all result from type I hypersensitivity. • It is caused upon contact with antigen against which the host has pre-existing IgE antibody.
IgE • IgE is present in very low levels in serum in most people • 50ng (ie 5 × 108gm) per ml. • It does not pass the placenta, although it is synthesized by the fetus. It does not fix complement, • Its' half life in serum is only 2-3 days but much of the IgE in the body is bound to high affinity receptors (FcepsilonRI), • in the bound state the half-life is ~3 weeks. • The high affinity FcepsilonRI receptors are found on mast cells and basophils. • Amounts in serum do not always reflect the degree of allergic sensitivity, because IgE antibody may sensitize tissues in the absence of a detectable excess free in the serum • The affinity of IgE for skin being so great that the site remained sensitized for 4 weeks or longer • Only a few molecules appear to be necessary for sensitization • the radioallergosorbent test (RAST)
Incidence and genetic susceptibility • 20-30% of the population exhibit type I hypersensitivity or atopic allergy to common environmental substances. • There is a genetic component to atopic allergy such that if both parents exhibit this susceptibility more than 2 • if neither parent has manifest allergies - less than half likely to when compared to the population as a whole. Some individuals have multiple and severe allergies, • typically both hayfever and eczema-these individuals are termed atopic and frequently have raised total serum IgE levels (10 -100 × normal). • There is a correlation between total [IgE] and atopy.
Mast cell mediators & Properties • Molecule effects • Primary mediators • Histamine Vascular permeability, sm contraction Serotonin vascular permeability, sm contraction • ECF-A eosinophilchaemotaxis • NCF-A neutrophilchaemotaxis • proteases mucus secretion, connective tissue degradation • Secondary mediators • Leukotrienesvascular permeability, sm contraction • Prostaglandins vasodilation, sm contraction, platelet activationBradykininvascular permeability, sm contraction • Cytokines numerous effects inc. activation of vascular endothelium, eosinophil recruitment and activation
Systemic anaphylaxis • Uncommon, but may follow • insect bites or stings, skin tests, • Administration of therapeutic sera or drugs, • muscle relaxants, anaesthetics, radiological contrast Media, • Manifested by respiratory distress due to bronchospasm or oedema of the mucosa of the larynx and bronchi, cutaneous changes varying from erythema to angio-oedema and urticaria, intestinal spasm accompanied by vomiting or diarrhoea, and shock. • Only one or a combination of these signs may be present, and the results vary from transient discomfort to rapid death.
Type II Hypersensitivity • Caused by specific antibody binding to cells or tissue antigens. • The antibodies are of the IgM or IgG classes • cell destruction by Fc dependent mechanisms either directly or by recruiting complement via the classical pathway. • the target cells are foreign to the host Except where the reaction is autoimmune. • Usually seen in blood transfusion recipients , • The classic ABO incompatibility reaction with IgM antibodies causing complement lysis of erythrocytes. • Rhesus disease (or haemolytic disease of the newborn) The IgG antibodies cause destruction of foetal RBC by antibody dependent cellular cytotoxicity (ADCC) are passively acquired by the host via the placenta.
Autoimmune hemolytic anemia • Goodpasture's syndrome • ErythroblastosisFetalis • Pemphigus • Pernicious anemia (if autoimmune) • Immune thrombocytopenia • Transfusion reactions • Hashimoto's thyroiditis • Graves' disease • Myasthenia gravis • Rheumatic fever • Hemolytic disease of the newborn
Type III Hypersensitivity • Mediated by immune complexes essentially of IgG antibodies with soluble antigens. • Only preformed complexes can bind to the low affinity FcgammaRIII. • soluble immune complexes (aggregations of antigens and IgG and IgM antibodies) form in the blood and are deposited in various tissues (typically the skin, kidney and joints) where they may trigger an immune response according to the classical pathway of complement activation
Type III Hypersensitivity • Immune complex glomerulonephritis • Rheumatoid arthritis • Serum sickness • Subacute bacterial endocarditis • Symptoms of malaria • Systemic lupus erythematosus • Arthus reaction • Farmer's Lung (Arthus-type reaction
Type IV Hypersensitivity • This is the only class of hypersensitive reactions to be triggered by antigen-specific T cells. • CD8+ cytotoxic T cells and CD4+ helper T cells recognise antigen in a complex with either type 1 or 2 major histocompatibility complex. • The antigen-presenting cells in this case are macrophages which secrete IL-12, which stimulates the proliferation of further CD4+ T cells. • CD4+ T cells secrete IL-2 and interferon gamma, further inducing the release of other Type 1 cytokines, thus mediating the immune response. • Activated CD8+ T cells destroy target cells on contact while activated macrophages produce hydrolyticenzymes and, on presentation with certain intracellular pathogens, transform into multinucleated giant cells.
Type IV Hypersensitivity • Contact dermatitis • Temporal arteritis • Symptoms of leprosy • Symptoms of tuberculosis • Transplant rejection • Coeliac disease
Post test • 13 A 35 year old man comes to see you. He is keen to have his thyroid function tested because his younger sister has just been diagnosed with hypothyroidism. His mother also suffered from this at an early age. You agree to do some blood tests. But within a few minutes of taking his blood he becomes acutely breathless with marked facial and tongue oedema. He tells you that he ate a prawn mayonnaise sandwich three hours earlier. • Shellfish allergy • Egg allergy • Vasovagal reaction • Latex allergy
The patient returns one year later. He was at a dinner party for his thirty-sixth birthday. After the dessert he felt tingling and tightness in his throat. He remembers the pudding was a fruit salad containing mostly banana and kiwi fruit. • What is the likely diagnosis? • a Cross reactive allergy • B Lactose intolerance • c Food intolerance • d Latex contamination of food • e Pesticide allergy • 15 What dose of adrenaline would you give the patient? • 0.5 ml intramuscular adrenaline 1:1000 • 0.5 ml subcutaneous adrenaline 1:1000 • 0.5 ml intravenous adrenaline 1:1000 • 0.5 ml intravenous adrenaline 1:10 000
He attends after yet another anaphylactic reaction. He treated himself with adrenaline and oral antihistamine, and after lying down for an hour he felt better. He asks you what the best site to inject his adrenaline is. • Where should you advise him to give his injection? • A The shoulder • b The buttock • c The upper arm • d The thigh • e The abdomen • When, if ever, should he use the second autoinjector? • After one minute if he does not improve • After five minutes if he does not improve • After 20 minutes if he does not improve • Never after a previous dose