Download
1 / 78
810 likes | 1.16k Views
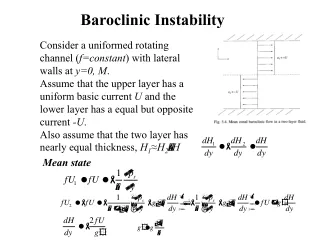
Shoulder Instability Basics. 18 February 2010. Contents. Terminology Anatomy Pathophysiology Evaluation Nonoperative Treatment Operative Treatment Treatment Course/Outcomes. Terminology. Laxity

E N D
Shoulder Instability Basics 18 February 2010
Contents • Terminology • Anatomy • Pathophysiology • Evaluation • Nonoperative Treatment • Operative Treatment • Treatment Course/Outcomes
Terminology • Laxity • Asymptomatic, passive translation of the humeral head on the glenoid unassociated with pain • Instability • Symptomatic pain/apprehension associated with excessive translation of the humeral head during active motion
Osteology • Glenoid version • 30o anterior • Humerus • Neck-shaft – 130o to 140o • Retrotorsion – 30o
Labrum • Fibrocartilaginous ring • Anchors capsuloligamentous structures • Deepens the glenoid • Doubles depth • Increases Surface area
SGHL • Most constant ligament – but variable thickness • 3 variations of origin • Inserts into top of humerus near tip of lesser tuberosity
Function-SGHL • Limit inferior translation and external rotation when arm is adducted • Limit posterior translation when the arm flexed, add, IR
Rotator Interval • Triangular area of tissue from supraspinatus superiorly to subscapularis inferiorly • Capsule thickened by SGHL & CH lig • Defects - ?? Significance
MGHL • Most variable • Sheetlike or cordlike • Originates from labrum or neck of glenoid just inf to SGHL • Inserts just medial to lesser tub closely opposed to subscap
Function • Limits anterior translation with 60o to 90o abduction and ER • Limits inferior translation with the arm adducted
IGHL • Anterior band, axillary pouch, posterior band • Originates from labrum/glenoid neck • Ant band – 2 to 4 o’clock • Post band – 7 to 9 o’clock • Inserts into anatomic neck humerus – 90o arc
Function • Limits anterior, posterior, and inferior translation depending on arm position • aIGHL limits AP translation in ext, pIGHL limits AP translation in flex
Instability Pathophysiology • Most motion of any joint • Dynamic and Static Restraints • Bankart lesion • Avulsion of IGHL & Labrum complex • HAGL
Stability • Static Factors • Articular Congruence • Articular Version • Glenoid Labrum • Capsule and Ligament
Pathology-version • Glenoid dysplasia • 1% to 3% of instability cases • Avoid surgery
Glenoid Rim Fracture • Reduces contact area and glenoid concavity • Less than 25% to 33% involvement not a problem if IGHL is reattached
Hill-Sachs Lesion • Impression fracture of posterolateral humeral head • Little consequence if soft tissue repair is performed • Some say greater than 30% involvement may lead to continued instability
Bankart Lesion • Detachment of anteroinferior labrum • IGHL is key • Essential lesion?? • Speer, et al: JBJS 76A, 1994
Capsular Injury • Acute tears • HAGL lesion • Plastic deformation • Bigliani, et al: JORS, 1992 • Circle concept • Need for capsular shift & failure of scope repairs
Stability • Dynamic Factors • Rotator Cuff • Biceps Tendon • Negative Pressure • Scapulothoracic motion
Rotator Cuff • Compression enhances conformity • Greater than static stabilizers • Coordinated contractions/steering effect • Supraspinatus most important • Dynamization
Scapulothoracic Motion • 2:1 glenohumeral to scapulothoracic motion • Scapulothoracic muscle (trapezius, serratus anterior) weakness produces winging less stable platform
Negative Intra-articular Pressure • -42 cm H2O in cadaver • Secondary to high osmotic pressure in interstitial tissues • Only clinically important in the arm at rest in adduction • with lax capsule or defect
Static Factors Articular Congruence Articular Version Glenoid Labrum Capsule and Ligament Dynamic Factors Rotator Cuff Biceps Tendon Negative Pressure Scapulothoracic motion Stability
TUBS Traumatic Unidirectional Bankart lesion Surgery AMBRII Atraumatic Multidirectional Bilateral Rehabilitation Inferior capsule Interval closure Instability Categories Thomas & Matsen, JBJS(1989)
Multidirectional Instability • Definition: • symptomatic increased translation of humeral head on glenoid. • Can be subluxated or dislocated, in three directions with reproduced symptoms with one or more of these directions.
MDI • No Single Etiology • Inherent Ligamentous Laxity • Trauma (Major/Repetitive Minor) • Scapular Mechanics
A Spectrum Traumatic Microtrauma Atraumatic Less laxity More laxity Unidirectional Multidirectional
Instability Classification: • Frequency • Direction • Degree • Etiology
Classification • Frequency • Acute • Recurrent • Fixed (chronic) • Cause • Traumatic event (macrotrauma) • Atraumatic event (voluntary, involuntary) • Microtrauma • Congenital condition • Neuromuscular condition (cerebral palsy, seizures)
Instability • Patient Evaluation
Position of Instability Traumatic/Atraumatic Onset of Symptoms===> Need for Reduction Psychiatric Component Family History Inf. Instab.– pain with carrying suitcase/shopping bags @ side Ant. Instab. – throwing, reaching objects – ABD/ER Post. Instab. – pushing heavy doors FF/IR History
Anterior Instability • Traumatic, acute, dislocation • Traumatic, acute, subluxation • Recurrent anterior instability • Chronic recurrent anterior dislocations • Chronic recurrent anterior subluxation • Fixed (locked) anterior dislocation
Posterior Instability • Traumatic acute dislocation • Traumatic acute subluxation • Recurrent posterior instability • Recurrent posterior dislocation • Recurrent posterior subluxation • Voluntary • Positional • Muscular • Chronic (locked) dislocation • <25% of articular surface • 25-40% of articular surface • <40% of articular surface
Multidirectional Instability • Type I - Global, atraumatic, instability • Type II - Anterior/inferior instability Macrotrauma in setting of hyperlaxity • Type III - Posterior/inferior instability Microtrauma in setting of hyperlaxity • Type IV - Anterior/posterior instability
Clinical Evaluation - History • Careful history is paramount • 1st episode of dislocation or subluxation • Degree of trauma - major, trivial, none • Dislocation vs. subluxation • Position of arm • More frequent episodes • Treatment
History - Present Symptoms • Arm “slips out” • Dead arm syndrome • Pain • Anterior/posterior pain = ant/post instability • Pain in context of arm position • Cocking vs. follow-through • Carrying heavy items • Secondary impingement • Popping/clicking
History- cont’d • Functional losses • ADLs vs. sports • Activity modification • Voluntary control • Positional • Muscular
Physical Examination • Inspection • Palpation/ROM Ligamentous laxity Load-Shift test Apprehension test/ Relocation test Sulcus sign RC pathology
Physical Examination • Examine both shoulders • Cervical spine • Generalized ligamentous laxity
Generalized Joint Laxity Tests • Passive thumb apposition • Passive finger hyper-extension so finger parallels forearm • Elbow hyper-extension >10 degrees • Knee hyper-extension >10 degrees • Excessive ankle dorsiflexion and foot eversion Carter and Wilkinson in (Brown CORR, 2000)
Shoulder Exam • Muscular atrophy • Tenderness • AC and SC joint tenderness • ROM - active & passive • Winging • Muscle strength • Supraspinatus - 90o scap elevation/45o int rot • Infraspinatus - 0o scap elevation/ -45o rot • Subscapularis - lift-off/ Napolean’s • Deltoid/Biceps/triceps/trapezius