Download
1 / 23
230 likes | 380 Views
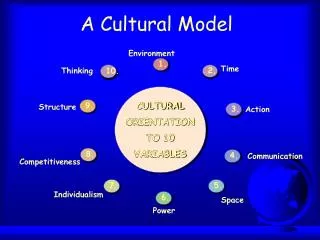
The Cultural Broker Model. From Paper to Practice. The Cultural Broker Model. Role Strain ↓ Bi-Cultural Competence ↓ Cultural Broker. Bi-Cultural Competence. Professional Culture + Community/Family Culture. Cultural Broker: Key Role of Home Visitor. Professional Culture ↕↕↕↕

E N D
The Cultural Broker Model From Paper to Practice
The Cultural Broker Model Role Strain ↓ Bi-Cultural Competence ↓ Cultural Broker
Bi-Cultural Competence Professional Culture + Community/Family Culture
Cultural Broker: Key Role of Home Visitor Professional Culture ↕↕↕↕ Community/Family Culture
Successful Site Characteristics • HVs Professionalism • HVs accept NFN model and parenting curricula • HVs “do curriculum” • HVs trust that supervisors share a deep concern for families • HVs strive to achieve bi-cultural competence • HVs express willingness to embrace cultural broker model
Recommendations from Report • “Generalist” v. “Specialist” role of HVs • From role strain to cultural broker • Organizational channels for HVs to participate in decision making • Substance abuse, domestic violence and poor mental health • Strengthen supervision • Career Ladders
Study Circles • What is it? • A democratic dialogue rooted in basic principles of action research designed to foster small group deliberation around common issues. • Program staff asked to volunteer: 94% participated
Recommendations provided to: • Professionalize the home visitor role • More clearly define and develop the supervisor role • Expand parenting curricula • Include home visitors in program decision-making • Better accommodate mothers’ schedules, especially working moms
Outcomes • Resulted in staff network meetings and CQI • Curricula Expanded • Clinical Supervisor • Home Visitor Training Increased • Eliminated credentialing and left Healthy Families
Revisiting the Cultural Broker Model Focus Group Study November and December, 2007
Background • New developmental stage & period of growth • New policies, training, curricula, supervision • Hartford is first city to “go to scale” in 2005
Focus Group Study: Nov/Dec 2007 • Purpose: Understand the decision-making process in identifying family needs and linking families to community resources • 4 focus groups: home visitors & supervisors • 8-10 participants/group, mix from different sites
Focus Group Discussions • Families with multiple problems • The “big three” risk factors • Creating change • The cultural broker model
Bridging Two Cultures …like I came from where a lot of these girls came from. Life was hard for me growing up…And I don’t get personal with them but I let them know ‘I’ve been there.’ [Another home visitor: Exactly.]...And I need to come off my professional pedestal, so to speak, and come down a couple of notches on her level and be like ‘Look.’ Get with the slang terms and everything for her to understand, where normally I don’t talk like that. I used to, but I am here now and it’s like just to show her ‘You can do it.’ Not to gloat to her. I don’t gloat to her, but I am like ‘Look. I been there. And she respects me...It works. It really does.
Generalist v. Specialist “That’s why so many families that come into the program new when we first start working with them there is no time to do any curriculum...That’s the last thing that they want to hear or see or read. They have so many other issues… They need to know where their next meal is coming from, like you said where they are going to lay their head. All that type thing. How are they going to take the baby to the doctor with no medical insurance, and all this type thing.”
Curriculum & ParentingOf Central Importance • They are not ready for it. But then you get overwhelmed when they are going on and on about ‘This is how I feel. This is what’s going on’. And you still have to try to find a way to bring it back to the child so that you are still being effective. • So then I take the book out. Parents as Teachers. The best thing…I like it a lot…That’s our Bible. [laughter from everyone]…And then I give them the handouts …
When and how is clinical supervision involved in the process? What is the supervisor’s role??
To Listen, Ask Questions “ [Clinical supervisors] have to know the family and they have to listen to what you say. Because [we] see themevery week. So it’s a person that’s really involved and really caring...Caring. That’s the key word. They have to be caring...And understanding, too.[Clinical supervisors] understand where the families are coming from. Not trying to put them where [they] think they should be,...”
And Provide Feedback • “With all the problems that [NFN families] have sometimes you don’t know whether you are coming or going. So you need someone that has their head on their shoulders and……says, ‘Why don’t we try this?’ “ • “we always keep her informed and we are in her office a lot, too, to try to get ideas or ask questions • Or by you telling [supervisor] what’s been going on to develop that plan, how can we be creative? How can we address the curriculum in a different way? How can we get the baby out of the parents’ room?
“Sometimes I feel really overwhelmed and drained and I sit with her and she can be very positive and help us a lot with our clients. [others agree]…And we do supervision every week. [laughs]…Oh, yeah. Because sometimes she has to tell us, ‘Okay, don’t take it personal’ about certain things... Let’s think about how we can work around it, how we can make it better.’ Yeah, supervision is crucial” And Support
Do you see change? Yes! • Relationships • Identifying problems with support and supervision • Figuring out effective strategies • Time and turning points
Cultural Broker Model as the mechanism for creating change • Improve support by focusing on the frontlines where staff and families come together Professional Culture ↕↕↕↕ Community/Family Culture • Experiences and knowledge that home visitors have of families and communities are a powerful resource for informing practice and policy
Questions for Discussion How can we improve the program model? What are the most challenging issues right now and is the program model effective in addressing them?