Download
1 / 50
500 likes | 679 Views

E N D
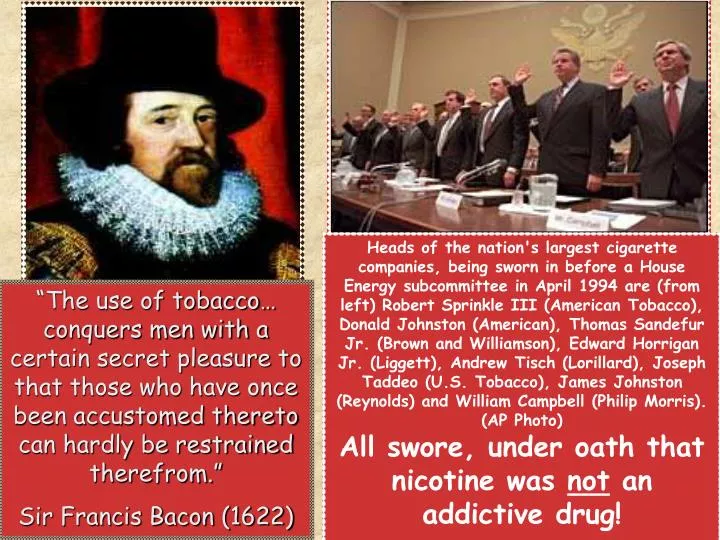
Heads of the nation's largest cigarette companies, being sworn in before a House Energy subcommittee in April 1994 are (from left) Robert Sprinkle III (American Tobacco), Donald Johnston (American), Thomas Sandefur Jr. (Brown and Williamson), Edward Horrigan Jr. (Liggett), Andrew Tisch (Lorillard), Joseph Taddeo (U.S. Tobacco), James Johnston (Reynolds) and William Campbell (Philip Morris). (AP Photo)All swore, under oath that nicotine was not an addictive drug! “The use of tobacco… conquers men with a certain secret pleasure to that those who have once been accustomed thereto can hardly be restrained therefrom.” Sir Francis Bacon (1622)
The Tobacco Consultation By Jay Taylor, RRT, TTS Your Host & Former Smoker! A.K.A.: How We Do It & What we teach your patients!
Getting Into The Room… The Approach Makes The Difference: Sometimes referred to a “The Dance!” Hi! My name is Jay (or Vickie, as the case may be), and I’m a Respiratory Therapist. Your doctor asked me to stop by and drop off some information, that might be helpful, should you ever decide you want to quit smoking. (Wait) I’m not here to tell you to quit… I’m here to show you how. Have you ever thought about quitting? What do you think?? (Let them talk)
Motivational Interviewing{ A very large portion of our consult involves talking one-on-one with the patient… partnering with them. Once they realize you aren’t a threat, and that you’re not preaching to them, they will usually open up... and then you can help them. The concept of MI is what helps us overcome the patient’s ambivalence - what has kept them from changing… the habit and the addiction of tobacco use (or any other addictive drug use). Think: ACTIVE LISTENING!
1.Express Empathy: 4 Principles of M. I. Best defined as acceptance. Through reflective listening (being able to repeat back what the patient has expressed), you come to understand where your patient is coming from without judging, criticizing or blaming. Acceptance is NOT the same thing as approval!
2. Develop Discrepancy: The goal here is to help your patient perceive for themselves a discrepancy between their present behavior and where they want to be. Their own goals, not someone else’s!
3. Roll With Resistance: Arguing with your patient to change their behaviors is the least effective thing you can do. Showing new ways to look at things and allowing your patient to find answers themselves (with your help) works best!
4. Support Self-Efficacy: This refers to encouraging your patients belief in the possibility of change; that they are in control and have control. Your expressed belief in the person’s ability to change becomes a self-fulfilling prophecy! NOT I will change you… but I will help you change!
For more information and education on the subject of Motivational Interviewing... MOTIVATIONAL INTERVIEWING Preparing People For Change By William R. Miller and Stephen Rollnick The Guilford Press (www.Guilford.com)
And Now… Let’s get into it! The Tobacco Consult
The History If we’ve learned anything about tobacco users, it’s that everyone is a little bit different! Kinda like snowflakes! So getting into the how’s, when’s and why’s of tobacco use will give you clues about how to treat the addiction.
What we need to begin the process is just plain data... Some of these questions are often asked out of order or even answered without asking. 8. Withdrawal Symptoms? Cravings Irritable Cranky Increased Eating Anxiety Depression Insomnia Nausea Lack Of Concentration Tobacco Dependence Interview Sheet Patient’s Name_________________________ 1 What form of tobacco do you use? Cigarettes Spit Tobacco Cigars/Pipe Other__________ 2.How much tobacco do you use daily? 3.How many years have you used tobacco. Quit Attempts: 4.Have you ever made a serious attempt to quit smoking (or chewing) in the past? None 1-2 Times 3+ Times 5.How long since your last attempt? 6.How long was your most successful attempt? 7.What methods/help have you tried? Cold Turkey Nicotine Nasal Spray Nicotine Patch Nicotine Lozenge Nicotine Inhaler Zyban/Wellbutrin/Bupropion Nicotine Gum Other_________________ 9. Reasons For Relapse: Crisis Chronic Stress Social Situation Withdrawal Symptoms Boredom Cravings Missed Cigarettes Couldn’t Resist Weight Gain Other:
Fagerstrom’s Scale of Addiction 1.How soon after you wake up do you have your first cigarette or chew? Within 5 minutes = 3 6 – 30 minutes = 2 31 – 60 minutes = 1 After 60 minutes = 0 2.Is the first cigarette/dip he day the most enjoyable? Yes = 1 No = 0 3.Do you smoke/chew more frequently in the morning than the rest of the day? Yes = 1 No = 0 4.Do you have cravings for tobacco when you are in places that you cannot smoke? Yes = 1 No = 0 5.If you are too sick to go about your normal activities, do you still smoke/chew? Yes = 1 No = 0 6.How many cigarettes/cans do you smoke/chew per day? 31+ 3 21-31 2 11-20 1 Score: _____ out of 10 <10 0 The Fagerstrom Scale of Addiction: Here’s what it means: Score: 0-3 Mildly Addicted 4-6 Moderately Addicted 7-10 Significantly Addicted (A 4 0r less will have less trouble quitting) (A 5 or more will have problems)
What’s Next? 10. How Motivated Are You To Quit? 1 2 3 4 5 How Would You Rate Your Ability To Quit? 1 2 3 4 5 Rationale:______________________ Motivation To Quit Ability To Quit They rate themselves which gives you lots of guidance. 12. Reasons: What Motivates You To Quit Smoking? Health Cost Family Social Pressure No Smoking At Work Other: Why do you want to quit. Is this for you or did someone tell you you had to? It’s going to be tougher yet if the patient tries and wants to quit while the spouse keeps puffing away.Offer help! 13. Other Tobacco users in your household? 14. Are they willing to make a quit attempt?
15. Barriers To Quitting: Dealing with stress. Withdrawal Weight gain Habit Fear of failure I LIKE to smoke Other: Basic Message: What gets in the way of quitting?Why not quit smoking? Any worries there? 16. Triggers: (What goes well with a cigarette? When do you smoke?) Alcohol Socializing After meals Being around smokers Automatic Driving Stress Coffee Other: Boredom Talking on Telephone Helping the patient have an idea of when they smoke will help later on in the consult. Information on quitting smoking is available in many Hispanic publications. We have also done consults with a telephone interpreter. 17. Barriers To Learning: None Other: Language Reading Age related Visual/Sensual I often tell patients today that setting a Quit Date is not as important as having a plan for Relapse Prevention in place! Quitting is pretty easy! Staying Quit is something else entirely! 18: Setting a QUIT DATE: Reminder: If using bupropion, set Quit Date 7-10 days after starting therapy. On Q.D. start NRT & Use Substitutes. Hard Candy, Toothpicks, Stick Cinnamon, Straws… etc.
N e x t... After we collect all of the patient history and information, the next step is a brief education about cigarettes or whatever form of tobacco the patient is using.
We talk about the 2 main components of tobacco smoke: TAR and NICOTINE Some 4,000 different chemicals... 60 Chemicals, known to cause CANCER in Humans Cyanide We set the NICOTINE aside for a moment and give a picture of what we call TAR! Toluene Formaldehyde Butane Arsenic Methane Benzine Ammonia Cadmium Carbon Monoxide Ethanol Acetone And that’s just for starters...
The Surprise! NONE of the chemicals listed in the previous slide are addictive at all! In other words, your brain never sends out a signal for you to run out and get some Formaldehyde… When you quit smoking, all of the BAD chemicals go away and you don’t miss them!!
Of that whole group of some 4,000 chemicals, you only miss 1when you quit smoking (or using tobacco) Yep!! It’s theNICOTINE! C10H14N2 C10H14N2
NICOTINEsets itself into your brain and receptor network (A4B2 Nicotinic Receptors) like a key in a lock or a baseball in a catchers mit. They fit perfectly! Why? Normally these receptors use acetylcholine. In truth, nicotine and acetylcholine resemble each other, but nicotine has a better and stronger fit!
Three Important Points:(To Drive Home) 2. Nicotine does not cause Heart Disease! 1. Nicotine does not cause Cancer! 3. Nicotine does not cause Lung Disease!
What NICOTINEdoes cause is:An Addiction To NICOTINE! Your brain and your Nicotinic Receptors send messages back and forth and when the message is that you need NICOTINE, much unhappiness ensues!! That’s where the cravings come from! When you’re addicted to nicotine, as 88% of tobacco users are, YOU’VE GOTTA HAVE IT!
So, since you need it, and since you’re human, you go looking for it in the easiest place to find it... …and that would be attached to 3,999 deadly chemicals!
How To Quit!What We Propose!! Huh?? Get and use all the NICOTINE your little heart desires… just don’t get it from smoking!
What we’re leading up to is using NRT or Nicotine Replacement Therapy! Nicotine replacement (SAFE Nicotine) is available in a number of forms, many not requiring a prescription (Well, cigarettes don’t require a doctor’s order) that you can use to relieve and remove the physical craving for tobacco products (nicotine).
Safenicotine is available by patch, gum, lozenge, inhaler and nasal spray. The patch, gum and lozenge can be purchased over the counter: without a prescription! (There is often a pause here,in the consult,while the patient explains why none of these products will work for them!) (We can usually explain why!)
A Little Patch of History For You... The first Nicotine Patch hit the market around 1992... A physicians prescription was necessary to obtain it. In 1994, an article appeared in the Wall Street Journal, citing anecdotal evidence that the nicotine patch might be dangerous, especially if one were to even accidentally smoke a cigarette while wearing it!! The source of this warning has been tracked to the big tobacco companies. The patch WAS dangerous… to their bottom line$$
Our friends, Phil Morris and old R. J. Reynolds have lots and lots of money! Last year, they spent around 36 MILLION dollars a day marketing their deadly product. Rumor has it that they don’t always tell the absolute truth when they talk, either... One of their most successful marketing techniques (ploys) is placing a little doubt in the minds of people, both professional and otherwise about the safety of NRT. Doubting the safety of Nicotine Patches has kept lots of people smoking and has kept many physicians from recommending them. Their campaign to keep people smoking, along with chemical efforts to make nicotine MORE addictive worked just fine, thank-you very much! The actual amount of nicotine per cigarette is higher than ever!!
The Facts Are: FACTS While Nicotine is most definitelynot good for you, using it by absorption, rather than by inhalation, is safe! And if the choice is to smoke or use nicotine replacement, guess which one is safer? Yes, you do have to keep in mind that Nicotine itself is not good for pregnant moms (Classified as a Class D drug) or moms that are nursing. And, Nicotine can impede the healing process following some surgeries! (Spinal fusion type.)
But! Butt? There are no published articles in any medical journals that show that using the patch to quit smoking will hurt you… at all! Please! Search your computers and medical files everywhere. This stuff is safe!! All Nicotine is not the same! You’re kidding! Really?
So… How do I use this patch thing?? And then what happens?? Some rather surprising information from The Mayo Clinic… The dose of NRT (nicotine replacement therapy) should match the amount of nicotine that you are already using!
Well… maybe not quite that many, but the Mayo Clinic model, which we use as the basis of our program, plus the education that we have received face-to-face from physicians and counselors during our training there, states clearly that using whatever amount of NRT you need to knock out cravings that occur with nicotine withdrawl, is how much you need! The Mayo Clinic teaches us “off label” instruction for using nicotine patches. The labels haven’t kept up with their research. Their basic teaching says: Patch To Match!
The Magic Formula One Cigarette equals One Milligram of NRT. Nicotine Patches come in 7mg, 14mg and 21mg doses. If you smoke 1 pack per day, that’s 20 cigarettes: One 21mg nicotine patch is a good STARTING DOSE! If you smoke 2 packs per day, that’s 40 cigarettes: Two 21mg nicotine patches is probably what you will need! If you smoke 3 packs per day… Guess What?
WOW! That sounds like a lot! We agree!
But… here’s a thought... If you had an infection of some kind, would you want just half of a dose of antibiotics?? I don’t think so! In the Mayo Clinic model, they cite cardiovascular patients wearing up to 3 patches at a time with no ill effect! Tobacco Abuse has been reclassified as a CHRONIC DISEASE. We must begin treating it as you would ANY chronic disease!
Along with our teachers and colleagues at the Mayo Clinic, Here’s what we recommend for our patients:Use as much NRT as you need to not have cravings, crabbiness, anxiety or any of the other classic symptoms of nicotine withdrawl. Use it long enough to let your nicotine receptors go back to doing what they are supposed to be doing. Then, wean it very slowly!
Weaning... After you find the dose that works for you, stay at that level for 4 weeks. Then begin weaning in increments of 7mg (The patch comes in 7, 14 and 21mg doses) spending 3-4 weeks at each level and always returning to a higher level if the symptoms sneak back up on you! Don’t be in a hurry! If you try to hurry, your receptors will make you crave and you will want to smoke.
So… What Then?? During the weaning period, you have a chance to address the triggers that are associated with lighting a cigarette. That cup of coffee, or mug of beer, or after a meal, or driving your car, or something stressful. These are the triggers that you have taught yourself to respond to with a cigarette!
You have carefully taught yourself to grab a cigarette when the bell rings (or the trigger appears!) It’s not all that hard to “un-teach” yourself. You have the 2 keys or weapons that you need to do this. #1 is MOTIVATION! You want to quit! #2 is NRT.You have this (on your arm, for example) already! Remember: The only real reason you smoke: the need for nicotine!
When you use the patch, even at the right dose, occasionally you may experience what we call a “breakthrough craving.” If it’s something you can’t handle on your own just by taking some deep breaths or some sips of water, using additional NRT from gum or lozenges is OK! OK! Sorry to beat this Nicotine thing to death, but just one more thing: The use of Nicotine Lozenges or Nicotine Gum can give you the extra edge you may need!
Other Stuff! Zyban… Wellbutrin… Bupropion... These medications are all the same thing: Bupropion. Wellbutrin is marketed as an antidepressant; Zyban was marketed as a stop-smoking drug; Bupropion is the generic equivalent of both. They act by affecting the dopamine producing area of the brain (the pleasure and reward center). In doing so, the need for nicotine may be reduced. Lots of potential side-effects! For some, it worked GREAT!! For others: not so much!
The Bupropion group, when they work, generally work better in combination with NRT, based on the Mayo model. But, you have to remember, this is an antidepressant. And while the side effects may or may not not be profound in most, occasionally they can bring on thoughts of suicide and can affect sexual things…L For a long, long time… this was all we had in our arsenal! …until very recently…J
Ta Daaah!! This year (2006) Pfizer introduced a drug that in a 2-year study of some 3600 motivated smokers, produced quit rates between 40 and 70%. The drug is called CHANTIX. It’s an A4B2 nicotinic receptor stimulant and nicotine blocker. Here’s how it works:
CHANTIX is a double-edged sword. The first function is to go up to the A4B2 receptor and tickle it a little bit. The receptor thinks this tickle is nicotine (because nicotine and acetylcholine resemble each other) and the receptor, in turn, creates a small dopamine (reward) response, which reduces cravings!
The second function is to actually block the nicotine from passing the receptor. It binds with the receptor. If the nicotine doesn’t get by, there is no nicotine response or thrill or kick or fun... Patients using CHANTIX report that they just get nothing from their cigarettes. It’s kind of like smoking a stick: nothing there! You Shall Not Pass!!
Dosing Chantix... Chantix is prescribed in one or two, 12-week periods. The 1st week is prescribed in the form of a starter pack. Starting Month: Day 1-3: ,you will take one 0.5 mg tablet; Day 4-7: you will take a 0.5 mg tablet twice daily; Day 8-28: you will take a 1 mg tablet twice daily Continuing Months: Week 2 to end of treatment: 1 mg tablet twice daily.
Drug Interactions? To date, studies have not shown any interactions with other medicines or drugs. Side Effects? Nausea was reported in about 30% of patients. It was described as mild and was generally prevented by taking the Chantix after a meal with a full glass of water. It gets better after a week. A small percentage (3%) had to discontinue use. Other side effects (to a lesser degree) include abdominal pain, flatulence, constipation, some insomnia and vivid dreaming. Restrictions? Dosage adjustments were made in patients with severe renal problems. Chantix was not studied for use in pregnancy (Class C) or with nursing Mom’s.
Relapse Prevention Failure? No… just normal! MOST tobacco users (nicotine addicts) try 7 or 8 times to quit using without success. Nicotine is the most addictive drug in the world, so what’s the surprise? Two BIG Tools! Number 1: Know that ALL relapse begins with 1 cigarette! Finding a way to avoid the first one is imperative! Number 2: When the chips are down and smoking seems to be the only option, begin using Nicotine Gum or Lozenges again!
So... Whether you use NRT, NRT with Bupropion, Bupropion alone or the new drug, Chantix… your ability to quit comfortably and your chances of success in quitting have increased many-fold. The key to the whole problem and to our program is: Motivation! Motivation: combined with Education & Medicine If you want this to happen, it will!
The Last Word comes from: Charles Harper, R.J. Reynolds Chairman "RJR Wins Fight",USA Today: B1, April 18, 1996 "If children don't like to be in a smoky room, they'll leave." When asked by a shareholder about infants, who can't leave a smoky room, Harper stated, "At some point, they begin to crawl."