Download
1 / 1
10 likes | 186 Views
Toxicity Patient reported Subjective Comparison to CTC-Grade burden informed consent. CRC actual survival CRC expected survival Non-CRC actual survival Non-CRC expected survival. Stomatitis Nausea Vomiting Diarrhea Fatigue Skin toxicity Neuropathy Alopecia. Survival in months.

E N D
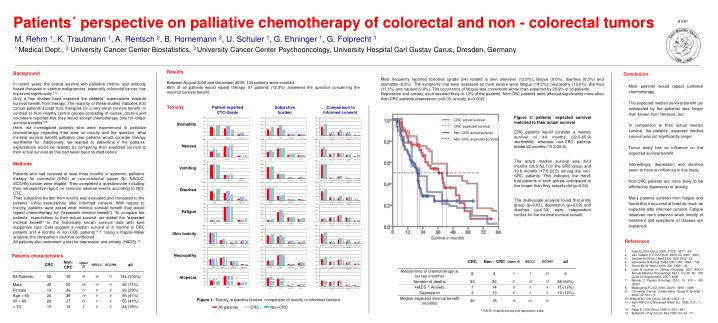
Toxicity Patient reported Subjective Comparison to CTC-Grade burden informed consent CRC actual survival CRC expected survival Non-CRC actual survival Non-CRC expected survival Stomatitis Nausea Vomiting Diarrhea Fatigue Skin toxicity Neuropathy Alopecia Survival in months Patients´ perspective on palliative chemotherapy of colorectal and non - colorectal tumors # 581 M. Rehm 1, K. Trautmann 1, A. Rentsch 2, B. Hornemann 3, U. Schuler 1, G. Ehninger 1, G. Folprecht 1 1 Medical Dept., 2 University Cancer Center Biostatistics, 3 University Cancer Center Psychooncology, University Hospital Carl Gustav Carus, Dresden, Germany Results Between August 2008 and December 2009, 134 patients were enrolled. 86% of all patients would repeat therapy. 97 patients (72.3%) answered the question concerning the minimal survival benefit. Background In recent years, the overall survivalwith palliative chemo- and antibody based therapies in various malignancies, especially colorectal cancer, has improved significantly.1-4 Only a few studies have explored the patients’ expectations towards survival benefit from therapy. The majority of these studies indicates that cancer patients accept toxic therapies for a very small survival benefit. In contrast to that, healthy control groups consisting of nurses, doctors and volunteers reported that they would accept chemotherapy only for longer survival benefits.5-8 Here, we investigated patients who were experienced in palliative chemotherapy regarding their view on toxicity and the question, what minimal survival benefit palliative care patients would consider therapy worthwhile for. Additionally, we wanted to determine if the patients´ expectations would be realistic by comparing their expected survival to their actual survival as this had never been studied before. • Conclusion • Most patients would repeat palliative chemotherapy. • The expected median survival benefit (as anticipated by the patients) was longer than known from literature, but: • In comparison to their actual median survival, the patients´ expected median survival was not significantly longer. • Tumor entity has an influence on the expected survival benefit. • Interestingly, depression and diarrhea seem to have an influence in this study. • Non-CRC patients are more likely to be afflicted by depression or anxiety. • Many patients suffered from fatigue and found that it occurred at least as much as expected after informed consent. Fatigue deserves more attention when toxicity of treatment and symptoms of disease are explained. Most frequently reported toxicities (grade 3/4) related to skin alteration (12.8%), fatigue (9.0%), diarrhea (8.5%) and stomatitis (8.3%). The symptoms that were assessed as most severe were fatigue (14.3%), neuropathy (12.0%), diarrhea (11.1%) and nausea (9.8%). The occurrence of fatigue was considered worse than expected by 29.9% of all patients . Depression and anxiety, each seemed likely in 12% of the patients. Non-CRC patients were affected significantly more often than CRC patients (depression: p=0.03; anxiety: p=0.002). Figure 2: patients´ expected survival matched to their actual survival CRC patients would consider a median survival of 44 months (22.0-65.9) worthwhile, whereas non-CRC patients stated 22 months (15.3-28.6). The actual median survival was 39.3 months (26.5-52.1) in the CRC group and 19.8 months (17.6-22.0) among the non-CRC patients. This indicates the trend, that patients of both groups anticipated to live longer than they actually did (p=0.06). The multivariate analysis found that entity group (p=0.03), depression (p=0.02) and diarrhea (p=0.03) were independent factors for the minimal survival benefit. Methods Patients who had received at least three months of systemic, palliative therapy for colorectal (CRC) or non-colorectal (upper GI, NSCLC, SCCHN) cancer were eligible. They completed a questionnaire including their retrospective report on common adverse events according to NCI-CTC. Their subjective burden from toxicity was evaluated and compared to the patients´ initial expectations after informed consent. With regard to toxicity, patients were asked what minimal survival benefit they would repeat chemotherapy for (“expected minimal benefit”). To compare the patients` expectations to their actual survival, we added the “expected minimal benefit” to the historically known survival data with best supportive care. Data suggest a median survival of 8 months in CRC patients and 4 months in non-CRC patients.9-12 Using a Kaplan-Meier analysis, the comparison could be conducted. All patients also underwent a test for depression and anxiety (HADS).13 • References • Kopetz J Clin Oncol 2009; 27(22): 3677 – 83 • Van Cutsem E J Clin Oncol 2006; 24: 4991 - 4997 • Sandler A N Engl J Med 2006; 355: 2542 - 50 • Vermorken B N Engl J Med 2007; 357: 1695 – 704 • Slevin ML Br Med J 1990; 300: 1458 – 60 • 6. Love N Journal of Clinical Oncology, 2007 ASCO Annual Meeting Proceedings Part I. Vol 25, No. 18S (June 20 Supplement), 2007: 4020 • 7. Balmer C Psycho-Oncology 2001;10: 410 – 418 (2001) • 8. Matsuyama R JCO 2006; 24(21): 3490 – 3496 • 9. Colorectal Cancer Collaborative Group P Br Med J 2000; 32: 531 – 5 • 10. Wagner A J Clin Oncol; 24(18): 2903 – 9 • Stell PM Clin Otolaryngol Allied Sci. 1983; 8 (1): 7 – 13 • Rapp E J Clin Oncol 1988; 6: 633 – 641 • Bjelland I J Psychosom Res 2002; 52: 69 - 77 Patients´characteristics • Figure 1: Toxicity, subjective burden, comparison of toxicity to informed consent • All patients CRC Non-CRC * HADS: hospital anxiety and depression scale