Download
1 / 16
160 likes | 676 Views
Pulmonary Zygomycosis. 47-year-old male Type II diabetes mellitus for 13 years Developed diabetic neuropathy and end-stage renal disease Renal transplantation and immunosuppression One month post-transplant Fever, chills, pleuritic chest pain

E N D
Pulmonary Zygomycosis • 47-year-old male • Type II diabetes mellitus for 13 years • Developed diabetic neuropathy and end-stage renal disease • Renal transplantation and immunosuppression • One month post-transplant • Fever, chills, pleuritic chest pain • Chest x-ray = cavitary lesion in right upper lobe • Sputum examinations negative for acid-fast bacilli • ATT initiated Chakrabarti et al. J ClinMicrobiol, 2010, 48(5): 1965-1969
Pulmonary Zygomycosis • ATT failed • Blood sugar • 153 – 226 mg/dl • Insulin therapy • Fine needle aspirate of lesion • Direct microscopy = no fungal elements • Fungal cultures were negative at 4 weeks • No improvement at 20 days • Open-lung biopsy of lesion, no mass noted Chakrabarti et al. J ClinMicrobiol, 2010, 48(5): 1965-1969
Pulmonary Zygomycosis Periodic acid-Schiff stain revealed acute inflammatory infiltrates and ribbon-like hyphae Chakrabarti et al. J ClinMicrobiol, 2010, 48(5): 1965-1969
Pulmonary Zygomycosis • Culture of the biopsy: • Fast growing, floccose whit colony turning grayish • Isolate identified as Rhizopus spp. Chakrabarti et al. J ClinMicrobiol, 2010, 48(5): 1965-1969
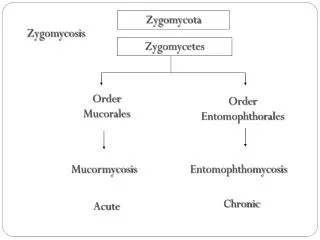
Zygomycosis • Epidemiology: • Ubiquitous • Usually – Rhizopus spp. • Others: Mucor, Absidia, Rhizomucor, and Cunninghamella • Virulence factors and pathogenesis: • Tissue necrosis suggests tissue destructive enzymes • Debilitated and immunocompromised • especially diabetic ketoacidosis • leukemias and lymphomas
Zygomycosis • Clinical Manifestation: • Route – inhalation • Incubation - ??? • Forms of infections: • Rhinocerebral zygomycosis – oropharyngeal, periorbital • paranasal sinus eye, brain • Risk factor = metabolic acidosis • Primary cutaneous zygomycosis (contaminated bandages) • Disseminated – fulminant and fatal, very poor prognosis • Cutaneous zygomycosis
Zygomycosis – Lab Diagnosis • Laboratory Diagnosis: • Monomorphic ,true mould • In tissue: • Try to get tissue for direct preps!! • Aseptatehyphae that branch at RIGHT angles, rare septations are possible (may see sporangial fruiting bodies) • In culture: • Several etiologies are differentiated by sporangia • Rhizopus spp.- Aseptatehyphae; sporangiophore arises from rhizoids, huge sporangia (100-300 um), filled with sporangiospores.
Zygomycosis - Treatment • Treatment: • Invasive disease is very difficult to treat/control • Amphotericin B … plus supplement abx • Surgical debridement • Immune reconstitution • Posiconazole appears to be active against most species
Pulmonary Zygomycosis • For our patient: • Liposomal Amphotericin B was administered • Striking improvement both clinical and radiological • No relapse at 5 months • Classical presentation of a susceptible diabetic host • Localized, primary pulmonary zygomycosis Chakrabarti et al. J ClinMicrobiol, 2010, 48(5): 1965-1969