Download
1 / 41
410 likes | 424 Views
OHSS Case Presentation & Discussion | Jindal IVF Chandigarh

E N D
OHSS Case Presentation &Discussion Dr. Tanya Chawla Dr. U. N. Jindal
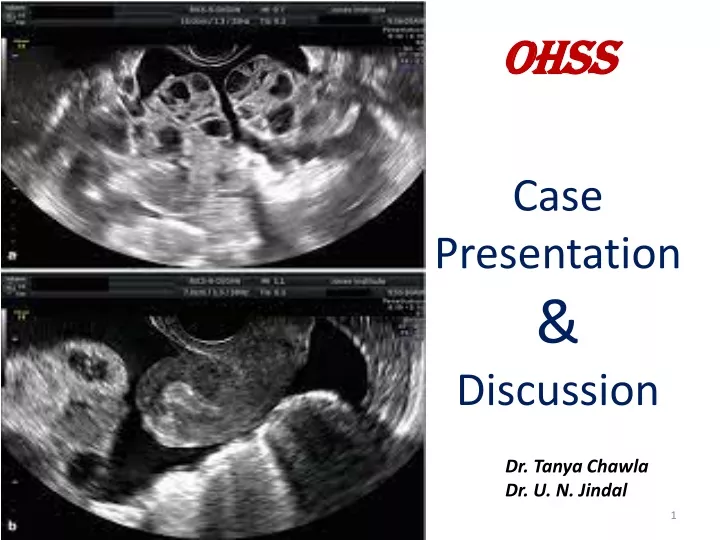
Mrs M, 30 yrs, married life – 5years, P1011 • FIRST VISIT : 17/08/21 for evaluation for OD. • LMP: 16/08/21; Prev cycles: 3-4/28, Reg • Obstetric history: P1011 P1 : FTNVD/ MCh /3yrs/A & H • A1 :Spontaneous abortion at ~ 6-7 weeks/medically managed • Past / Family history : Not significant TVS Uterus AV, Normal size RO : Normal; AFC : 5-6 LO : Normal; AFC : 6-7 Injection Ovurelix 0.25mg S/C on 17/08 and 18/08. Routine Investigations : Normal AMH : 3.47ng / mL DECLARED FIT FOR PROCEDURE .
Stimulation From 19/08/21 • ANTAGONIST PROTOCOL • Inj RECAGON 200IU + Inj MENODAC 75 IU (5 days) • Inj RECAGON 200IU + Inj MENODAC 150 IU + Inj OVURELIX (next 5 days) • Trigger : InjhCG 5000IU + InjOvitrelle 250ug (29/08/21) • OPU done on 31/08/21: 4RO + 5LO = 9 oocytes retrieved • Pt discharged on the same day
GENERAL EXAMINATION • Weight : 59.2kg • Vitals stable • SPO2 – 99% (room air) • RS - B/L Chest clear • P/A : Soft, NAD; AG : 36.5 in USG : Hyperstimulated ovaries with fluid in POD • FOLLOW UP: DAY 8 Pt came on D8 of OPU with complaints of : • Abdominal distension since 5-6 days • Vomiting since 2 days • No breathing difficulties • No c/o decreased urine output Provisional Diagnosis: Mild Late Onset OHSS • ADMITTED: • TREATMENT STARTED : GnRH Antagonists (InjOvurelix 0.25mg) x 6 days • Dopamine agonists (T. Cabergoline 0.5 mg) x 6 days • Thromboprophylaxis (InjEvaparin 40mg ) • I/V antibiotics (InjCeftriaxone 1gm) • Antiemetics & PPIs
RCOG : • Paracentesis (Indications) • Severe abdominal distension & pain (Ascitis) • SOB and respiratory compromise (Ascitis & ↑ IAP) • Oliguria despite adequate volume replacement (↑ IAP reduced renal perfusion) POST PROCEDURE Intravenous colloid therapy to be considered for large volumes of fluid removed .
Large volume paracentesis with colloid replacement is rapid, safe, and effective • 4–6 l/day • Albumin infusion (8 g/litre of ascitesremoved) Commonest site : ~ 15 cm lateral to umbilicus For diagnostic purposes, 10–20 ml. Sent for Cytology, culture, biochemistry Informed consent Total paracentesis is generally safer than repeated paracentesis Failure to give volume expansion circulatory dysfunction impairment of renal function & electrolyte disturbances Albumin or Artificial plasma expanders. .???? Albumin is more effective in preventing hyponatraemia VS other plasma expanders. Amount..?? Time…?? Route..?? Interval..?? Till further studies: albumin remains the plasma expander of choice when large volume (>5 litre) paracentesis <5 litre : Synthetic plasma expander; does not require albumin
- Removal of 4–6 litres is usually enough for symptomatic relief (usually only removing 2-4 litres maximum) - Removal of more than 4-6 litres increases the risk of hypovolemia and adverse effects.
CLASSIFICATION : TIME OF ONSET • LATE • Typically presents ≥ 10 after the hCG injection • Due to endogenous hCG derived from an early pregnancy • More prolonged and severe • EARLY • Usually presents between 3 - 7 days of the hCG injection • Due to excessive ovarian response
Ascitic fluid analysis • Culture : sterile • Cytology : Moderate cellularity predominantly polymorphs with few mesothelial cells and lymphocytes; Negative for malignant cells • Routine
Follow up : Day 17 of OPU • General & Systemic examination • Weight : 69.5 kg • Vitals stable • SPO2 – 96% (room air) • RS - B/L Chest clear • P/A : Distension + AG : 39.5 in • USG : Enlarged ovaries with fluid all around the uterus and adnexa; Ascitis ++ • READMITTED • Routine investigations sent C/o: Abdominal pain and distension • Pedal oedema • BhCG : 83 • - Ascitic Tapping • Pleural tapping • Albumin infusion • - InjMethotrexate 75mg IM • InjPiptaz 4.5gm • Diuretics • TREATMENT STARTED : • - Thromboprophylaxis (InjEvaparin ) • I/V antibiotics (InjCeftriaxone 1gm) • Antiemetics & PPIs
RCOG : FLUID REPLACEMENT • Oral route, guided by thirst : most physiological approach (Fluid intake of at least 1 litre / day ) • I/V Fluids: For acutely dehydrated patients OR Poor oral intake (AVOID vigorous I/V fluid therapy : may worsen ascites) • Evidence to support specific regimen of fluid replacement : Lacking
FLUID REPLACEMENT……continued CYSTALLOIDS (NS, DNS): Fluids of choice for INITIAL Correction Infused @ 125- 150 mL/h with periodic urine output monitoring. Alternate colloid solution (HETASTARCH, ALBUMIN, FFP) • Urine output < 1000ml per 24 hours • OR • POSITIVE fluid balance >1000ml over 24 hours REVIEW TO ASSESS SEVERITY Persistent haemoconcentration OR Low urine output INDICATES NEED OF MULTIDISCIPLINARY ASSISTANCE ± INVASIVE HAEMODYNAMIC MONITORING
Mechanisms: • Binds & inactivatiesvasoactive peptides VEGF and factors related to RAS. • ↑ plasma oncotic pressure Counteracts the permeability effect of angiotensin II drawing fluid from the third compartment. Effective plasma expander when crystalloids fail to achieve hemodynamic stability. Human albumin solution 20% in doses of 50–100 g, infused over 4 hours and repeated 4- to 12-hourly. Fresh frozen plasma may be used alternatively • Note: • Albumin is a blood-derived product • Allergic reactions • Anaphylaxis • Transmission of viral or unidentified diseases.
LASILACTONE • GRADE 2 ASCITES (FIRST EPISODE) : SPIRONOLACTONE • HYPERKALEMIA Add FUROSEMIDE • RECURRENT ASCITES : SPIRONOLACTONE + FUROSEMIDE • - LOOP diuretics (Furosemide) alone are ineffective. • - Spironolactone alone may take longer (look for Hyper K+) • - Combination therapy has more rapid effect (check RFTs) • Diuretics contraindicated due to intravascular volume depletion. Hypothetical risk for further hemoconcentration. • advantage of preventing oliguria/anuria • Use only after correction of intravascular volume and rehydration with 2 L of IV saline/day correct hemoconcentration and also prevent renal failure. • Recommendation to use furosemide only after the hematocrit level has decreased to 38% or lower. • Diuretics should be avoided : further deplete intravascular volume • Role in a multidisciplinary setting if oliguria persists despite adequate fluid replacement and drainage of ascites DIURETICS
DEFINITION An iatrogenic complication of assisted reproduction technology. Characterized by cystic enlargement of the ovaries and a fluid shift from the intravascular to the third space due to increased capillary permeability and ovarian neoangiogenesis.
Systemic condition; hcg dependent Ongoing hcg stimulation (pregnancy) Proinflammatory mediators from GC : VEGF, IL-6, 1b, TNF-a, Angiotensin II, IGF-1, PDGF & RAS (proangiogenic) Arteriolar vasodilation + Increased capillary permeability
Fluid shift from intravascular to extra- vascular spaces • Manifests as Ascites; less commonly as pleural and pericardial effusions HYPOVOLAEMIC HYPONATREMIC STATE
Young Age RISK FACTORS AFC > 24 Low BMI PCO Pregnancy AMH > 3.4ng / mL GnRH agonist protocol E2 > 3500pg / mL High dose Gn > 25 follicles hCG trigger > 24 oocytes retrieved
MANAGEMENT Diagnosis Classify as per severity.
MILD • MODERATE • Selective Cases Of SEVERE OHSS SELF LIMITING : resolves in 7-10 days Who do not conceive :Resolves by next menses Who conceive: symptoms may extend till end of 1st TM O P D • OUTPATIENT MANAGEMENT: • Easy access to hospital facilities • -Ensure adherence • COUNSELLING • -SYMPTOMATIC TREATMENT • PAIN RELIEF (AVOID NSAIDS) • THROMBOPROPHYLAXIS (SEVERE OHSS) • PARACENTESIS (to prevent progression)
ADMIT SEVERE CRITICAL : ICU / CCU MONITORING • TREATMENT MODALITIES • Intravenous hydration • Pain relief • Thromboprophylaxis • Paracentesis • Albumin infusion • GnRH antagonists • Diuretics • LABORATORY • CBC with Hct • RFT • LFT • Sr electrolytes • Coagulation profile • B-hCG • USG pelvis • CXR CLINICAL -Body weight -Abd girth -Fluid intake -Urine output -Vitals - Saturation
SEVERE / CRITICAL PROTHROMBOTIC STATE MODERATE EVALUATE for Risk factors Antiembolism stockings / LMWH THROMBOPROPHYLAXIS • DURATION • INDIVIDUALISED • Risk factors • Conception ± • Till end of 1st TM LOOK FOR - Symptoms and signs of VTE - Unusual neurological symptoms (even after several weeks of apparent improvement in OHSS)
ANALGESICS • Acetaminophen (paracetamol) and/or opioid analgesics. • AVOID NSAIDs with antiplatelet properties; may worsen renal function. ANTI-EMETICS • Severe pain : Rule out • ovarian torsion or rupture • coincident problem such as ectopic pregnancy or pelvic infection.
GnRH Antagonists Duration: 6-7 days • MECHANISM: • - Direct action on the ovary. • GnRH receptors are present in granulosa-lutein cells. • GnRH antagonists reduces mRNA expression for VEGF and VEGF receptor in the hyperstimulated ovaries. GnRH antagonist administration in established severe early OHSS may result in quicker regression.
DOPAMINE AGONISTS Dopamine-receptor agonist such as cabergoline may result in a reduction of VEGF production There is good evidence that dopamine agonist starting at the time of hCG trigger for several days reduces the incidence of OHSS. Gardener’s Textbook of ART Use of cabergoline from day of hCG administration to six days post-oocyte retrieval > 50% reduction in incidence of moderate OHSS
BASED ON CLINICAL CONDITION: • - Arterial blood gases • - ECG / 2D echo • - Chest X-ray • Ultrasound pelvis • B-hCG - C-reactive protein levels : role in severity MONITORING DAILY BASIS: • Vitals • Body weight • Abdominal girth • Fluid intake and Urine output • LABORATORY • Full blood count with Hct • Serum electrolytes • Osmolality and Renal & Liver function tests • Coagulation profile • SIGNS OF WORSENING • ↑ abdominal distension & pain • SOB • Tachycardia or hypotension • ↓ urine output (< 1000ml/24 hrs) OR Positive fluid balance (>1000 ml/24 hrs) • Wt gain & increased AG • ↑ Hct ( > 45% ).
SURGICAL INTERVENTION Only indicated in patients with coincident condition • adnexal torsion • ovarian rupture • ectopic pregnancy
PREVENTION Type of Stimulation Protocol : GnRH agonist vs. GnRH antagonist protocols Choice of Trigger for Final Oocyte Maturation
PREVENTION Cryopreservation : Coasting : • Involves withdrawing exogenous gonadotrophins and postponing hCG administration until the patient’s serum estradiol (E2) level decreases to a ‘safer’ level in patients who are anticipated to be at risk of developing severe OHSS There is insufficient evidence to recommend coasting for the prevention of OHSS
ASPIRIN:Women taking aspirin had a lower incidence of severe OHSS requiring hospital admission (antiplatelet) METFORMIN :Reduces intraovarianhyperandrogenism reduces the number of non- periovulatory follicles reduces estradiol secretion There is good evidence that metformin decreases the risk of OHSS risk in PCOS patients. DOPAMINE AGONISTS : There is good evidence that dopamine agonist starting at the time of hCG trigger for several days reduces the incidence of OHSS I/V CALCIUM: (10 mL of 10% calcium gluconate in 200 mL NS) on the day of OPU & for next 3 days can decrease OHSS risk. Calcium inhibits cAMP-stimulated RAS ↓ VEGF production
Autotransfusion of ultrafilteredasciticfluid into the venous circulation [CART] • reduced haemoconcentration, • improved urine output • quicker recovery • Extent of benefit of this treatment is doubtful…!!!!! • Studies describe autotransfusion of concentrated ultrafiltered ascetic fluid protein • aim to replenish the woman’s albumin levels using her own protein, reducing the risk of infection and allergic reaction to exogenous albumin. • SU5416 • -Thromboembolism • Vomiting • Interference with early pregnancy development • QUINAGOLIDE : DR-2 agonist • DOXYCYCLINE : inhibits angiogenesis
