Download
1 / 89
1.02k likes | 1.93k Views
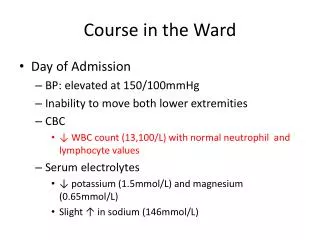
Maternal Collapse in labour ward. Dr . J. Edward Johnson. M.D., D.C.H. Asst. Professor , Dept. of Anaesthesiology , KGMCH. DISCUSSION. 1.CAUSES OF MATERNAL COLLAPSE 2. DIAGNOSIS OF - ETIOLOGY - COMPLICATION

E N D
Maternal Collapse inlabour ward Dr . J. Edward Johnson. M.D., D.C.H. Asst. Professor , Dept. of Anaesthesiology, KGMCH.
DISCUSSION 1.CAUSES OF MATERNAL COLLAPSE 2. DIAGNOSIS OF - ETIOLOGY - COMPLICATION 3. MANAGEMENT - RESUSITATION (CPR) - TREATMENT OF ETIOLOGY 4. WORK FORCE / PROTOCALS
CAUSES OF MATERNAL COLLAPSE Haemorrhage (APH, PPH) Pul.Embolism Amniotic Fluid Embolism Pre-eclampsia/eclampsia Cardiac (Valvular HD) Syncope Sepsis Respiratory
Causes of Collapse 4 H’s: Hypoxia Hypovolaemia (bleeding/block) Hypothermia Hypo/hyperkalaemia (metabolic) 4 T’s: Thromboembolic (PE or AFE) Toxic/therapeutic (local anaesthetic) Tension pneumothorax Tamponnade Eclampsia
Leading causes of Direct Deaths(Mortality rates/Million Maternities)
Haemorrhage is the major cause of maternal collapse in labour ward
Postpartum Hemorrhage “Obstetrics is Bloody Business”* *Cunningham, et. al: Williams Obstetrics, 21st ed., 2001
DIAGNOSIS OF ETIOLOGY
Postpartum Hemorrhage
Diagnosis ofCauses Postpartum Hemorrhage • Retained placenta • Placenta Accreta • Uterine atony • Vaginal and cervical laceration • DIC, AFE • Factor disorder • Uterine rupture / Uterine inversion
MANAGEMENT RESUSITATION OF Haemorrhagic Shock & Cardiac Arrest -(CPR)
Classification of Haemorrhage Baker R, Obstet Gynecol Annu, 1997
ASSESSMENT OF BLOOD LOSS AFTER DELIVERY Difficult Mostly Visual estimation (So, Subjective & Inaccurate) Underestimation is likely Clinical picture -Misleading Our Mothers-Malnourished, Anaemic, Small built, Less blood volume
SYMPTOMS & SIGNS Recognition is late - >30% B Vol loss
Modified Early Warning Scoring System (MEWS) MEWS calculated from 5 physiological variables • Mental response • Pulse rate • Systolic BP • Respiratory rate • Temperature
Modified Early Warning Scoring System (MEWS) The senior nurse would call the doctor for three or more of the following criteria: • Respiratory rate of ≥25 or <10 breaths per minute. • Arterial systolic blood pressure of <90mmHg. • Heart rate of ≥110 or <55 beats per minute. • Not fully alert and orientated. • Oxygen saturation of <90 per cent. • Urine output over the last four hours of <100ml. • Respiratory rate ≥35 breaths per minute or a heart rate ≥140 beats per minute.
Vigilance is great, but you have to remember that studies show the half-life of vigilance is about 15 minutes. Author unknown
DO NOT UNDERESTIMATE BLOOD LOSS Clinical Features of Shock
Goals of Therapy Maintain the following: Systolic pressure >90mm Hg Urine output >0.5 mL/kg/hr Normal mental status Eliminate the source of hemorrhage Avoid overzealous volume replacement that may contribute to pulmonary edema
Management of Obstetrical Hemorrhage Oxygen by mask 10 liter/min. – to keep O2 saturation > 94% 1st IV Line: Ringer Lactate with Pitocin 20-40 units at 1000 ml/ 30 minutes 2nd IV Line: 18 G IV: warm RL - administer wide open Sample blood; CBC, fibrinogen, PT/PTT, platelets, T&C and order 4u PRBCs Monitor I&O, urinary Foley catheter Get help -Senior Obstetrician, Anesthesiologist, Interventional Radiology, Intensivist, Haemotologist etc.
Management of Obstetrical Hemorrhage LR or NS replaces blood loss at 3:1 Volume expander 1:1 (albumin, hetastarch, dextran) Anticipate Disseminated Intravascular Coagulapathy (DIC) Verify complete removal of placenta, may need ultrasound Inspect for bleeding -episiotomy, laceration, hematomas, inversion, rupture Emperic transfusion -2 u PRBC; FFP 1-2 u/4-5 u PRBC -Cryo 10 u, -Uncrossed (O neg.) PRBC – For emergency Warm all blood products and I.V.infusions -prevent hypothermia, coagulopathy, arrhythmias
Blood Component Therapy Fresh Frozen Plasma INR > 1.5 - 2u FFP INR 2-2.5 - 4u FFP INR > 2.5 - 6u FFP Cryoprecipitate ( 1u/ 10Kg ) Fibrinogen < 100 mg/dl – 10u cryo Fibrinogen < 50 mg/dl – 20u cryo Platelets Platelet. count. < 100,000 – 1u plateletpheresis Platelet. count. < 50,000 – 2u plateletpheresis
Target Values Maintain systolic BP>90 mmHg Maintain urine output > 0.5 ml per kg per hour Hct > 21% Platelets > 50,000/ul Fibrinogen > 100 mg/dl PT/PTT < 1.5 times control Repeat labs as needed – every 30 minutes
Management of Major Obstetric HaemorrhageRecombinant factor VIIa (rFVIIa)
rFVIIa works at the site of vascular injury, where tissue factor (TF) is expressed and activated platelets aggregate. rFVIIa The fibrin clots formed in the presence of of a high thrombin concentration have a different architecture that is stronger and more resistant to degradation by fibrinolytic enzymes. Fibrin Fibrinogen Thrombin Here it enhances localized thrombin generation and the formation of a stable fibrin-based clot. Va rFVIIa Xa In pharmacological doses rFVIIa binds directly to the activated platelet surface. Prothrombin X
Recombinant factor VIIa • It is not licensed for use in obstetric haemorrhage and there have been no randomised contolled trials for its use in this situation • The dose is approximately 90μg/kg. • Its efficiacy is dependent on • -normothermia, • -non-acidotic milieu • -adequate levels of fibrinogen (> 1.0-1.5gr) -platelets (> 50,000) • A relatively early itervention to control PPH appears to be crucial for the success of rVIIa
Management of Major Obstetric Haemorrhage - rFVIIa rFVIIa will not replace ligatures in controlling bleeding from damaged or torn vessels. Tobe effective there must be adequate circulation delivering platelets and fibrinogen to the site of bleeding. You should make your best efforts to correct acidosis and hypothermia.
TREAT THE ETIOLOGY OF PPH
TEAM - Obstetrician, - Anesthesiologist, - Haematologist and - Blood Bank Correction of hypovolaemia Ascertain origin of bleeding Ensure uterine contraction Surgical management Management of special situation MANAGEMENT OF PPH
Massive Obstetric Haemorrhage Treatment • Medical • Surgical • Blood Component Therapy • Post Treatment Care
Massive Obstetric Haemorrhage Medical Volume Replacement (Crystalloid,Colloid) Blood (O –tive, Group Specific, X Matched) Coagulation Support (FFP, Cryoprecipitate, Platelets) Inotropic Support Uterine Massage / Compression Uterotonic Agents (Syntocinon ,Ergotamine, CarboprostMisoprostol ) Temperature Active Warming
Massive Obstetric Haemorrhage Surgical • EUA Repair • Uterine Tamponade (78%) • B-Lynch Suture (81%) • Arterial Ligation • Radiological Arterial Embolisation • Hysterectomy ( 12%)
Treatment of PPH: Hysterectomy Early Decision A conservative option should be quickly efficacious The addition of successive conservative approaches is hazardous - Risk of delaying radical treatment Placenta accreta is a frequent cause of failure of conservative Treatments Hysterectomy may be a life-saving procedure in case of - Failure of conservative approach - Uterine rupture - Placenta accreta
Strategically difficult in many centers Selective Angiographic Embolization (SAE)
Pulmonary Embolism
Pulmonary Embolism Pulmonary embolism, along with amniotic fluid embolism, accounts for the leading cause of maternal mortality in the United States (Koonin, et al; MMWR)
DVT: Key Facts • 40% of asymptomatic patients with DVT have radiographically documented pulmonary embolism • DVT of pelvic venous system is often an asymptomatic condition until clinical pulmonary embolism develops • Untreated pulmonary embolism mortality is up to 30%. Treated mortality is 3% (Moser et al, 1994; Cunningham et al, 1997; Toglia & Weg, 1996)
The Wells score • clinically suspected DVT - 3.0 points • alternative diagnosis is less likely than PE - 3.0 points • Tachycardia - 1.5 points • immobilization/surgery in previous four weeks - 1.5 points • history of DVT or PE - 1.5 points • hemoptysis - 1.0 points • malignancy (treatment for within 6 months, palliative) - 1.0 points Traditional interpretation • Score >6.0 - High • Score 2.0 to 6.0 - Moderate • Score <2.0 - Low Alternate interpretation • Score > 4 - PE likely. Consider diagnostic imaging. • Score 4 or less - PE unlikely. Consider D-dimer to rule out PE.
Diagnosis of Pulmonary Embolism • D-dimer (0-300 ng/ml as normal) • Chest X-ray • ECG • Arterial blood gas • Ventilation-perfusion scintography • Angiography • Thoracic enhanced CT (64 slices MDCT) • Extremity Doppler
Chest X-Ray Findings inPE: • Hampton’s Hump: pleural based density at CPJ • Westermark’s Sign: peripheral aligemia with proximal vessel dilatation • Most common finding is normal X-Ray (30%)!
ECG Changes in PE: • p-pulmonale, RBBB, RAD •S1 Q3 T3 classic signs -large S wave in lead I -a large Q wave in lead III and -an inverted T wave in lead III • New Onset A-Fib • Most common finding is normal (or sinus tach) ECG
Radiographic Diagnosis ofPulmonary Embolism DuringPregnancy: • Ventilation/Perfusion (V/Q) Scanning • Pulmonary Angiography • Spiral/Helical CT
Treatment- PulmonaryEmbolism in Pregnancy • Anticoagulation is mainstay of pharmacotherapy • Supportive care should not be forgotten during the rush to diagnose and treat
Venous Air Embolism • During the repair of hysterotomy wound • Exteriorization of the uterus and traction on the wound edges increases the risk • Trendelenburg position to be avoided • Abdominal and Uterine incision always below heart • CVP, High Uterine wound Air Embolism
Amniotic Fluid Embolism “Anaphylactoid syndrome of pregnancy"