Download
1 / 1
10 likes | 406 Views
43. Inpatient Rehabilitation Trends in the Morbidly Obese Population Paul Thananopavarn MD, Monica Carrion-Jones MD, Ann Nunez MD, Stephanie Slayton PT, Daniel Wong PhD Pitt County Memorial Hospital/East Carolina University Brody School of Medicine, Greenville, NC. Abstract

E N D
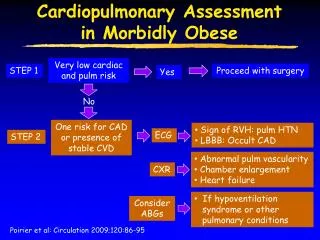
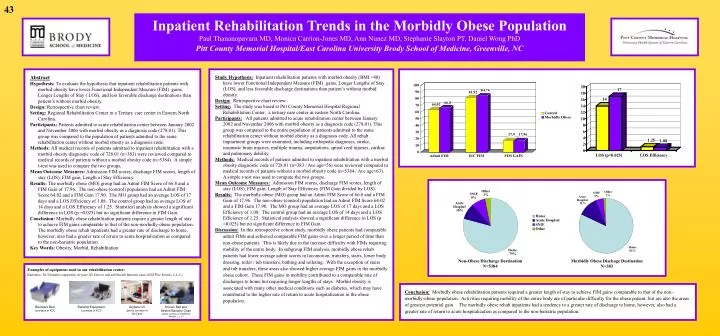
43 Inpatient Rehabilitation Trends in the Morbidly Obese Population Paul Thananopavarn MD,Monica Carrion-Jones MD, Ann Nunez MD, Stephanie Slayton PT, Daniel Wong PhD Pitt County Memorial Hospital/East Carolina University Brody School of Medicine, Greenville, NC Abstract Hypothesis: To evaluate the hypothesis that inpatient rehabilitation patients with morbid obesity have lower Functional Independent Measure (FIM) gains, Longer Lengths of Stay ( LOS), and less favorable discharge destinations than patient’s without morbid obesity. Design: Retrospective chart review. Setting: Regional Rehabilitation Center in a Tertiary care center in Eastern North Carolina. Participants: Patients admitted to acute rehabilitation center between January 2002 and November 2006 with morbid obesity as a diagnosis code (278.01). This group was compared to the population of patients admitted to the same rehabilitation center without morbid obesity as a diagnosis code. Methods: All medical records of patients admitted to inpatient rehabilitation with a morbid obesity diagnostic code of 728.01 (n=383) were reviewed compared to medical records of patients without a morbid obesity code (n=5384). A simple t-test was used to compare the two groups. Mean Outcome Measures: Admission FIM scores, discharge FIM scores, length of stay (LOS), FIM gain, Length of Stay Efficiency. Results: The morbidly obese (MO) group had an Admit FIM Score of 66.8 and a FIM Gain of 17.96. The non-obese (control) population had an Admit FIM Score 64.02 and a FIM Gain 17.90. The MO group had an average LOS of 17 days and a LOS Efficiency of 1.08. The control group had an average LOS of 14 days and a LOS Efficiency of 1.25. Statistical analysis showed a significant difference in LOS (p =0.025) but no significant difference in FIM Gain. Conclusion: Morbidly obese rehabilitation patients require a greater length of stay to achieve FIM gains comparable to that of the non-morbidly-obese population. The morbidly obese rehab inpatients had a greater rate of discharge to home, however, also had a greater rate of return to acute hospitalization as compared to the non-bariatric population. Key Words: Obesity, Morbid, Rehabilitation Study Hypothesis:Inpatient rehabilitation patients with morbid obesity (BMI >40) have lower Functional Independent Measure (FIM) gains, Longer Lengths of Stay (LOS), and less favorable discharge destinations than patient’s without morbid obesity. Design: Retrospective chart review. Setting: The study was based at Pitt County Memorial Hospital Regional Rehabilitation Center, a tertiary care center in eastern North Carolina. Participants:All patients admitted to acute rehabilitation center between January 2002 and November 2006 with morbid obesity as a diagnosis code (278.01). This group was compared to the entire population of patients admitted to the same rehabilitation center without morbid obesity as a diagnosis code. All rehab impairment groups were examined, including orthopedic diagnoses, stroke, traumatic brain injuries, multiple trauma, amputations, spinal cord injuries, cardiac and pulmonary debility. Methods:Medical records of patients admitted to inpatient rehabilitation with a morbid obesity diagnostic code of 728.01 (n=383 / Ave age=56) were reviewed compared to medical records of patients without a morbid obesity code (n=5384 / Ave age=63). A simple t-test was used to compare the two groups. Mean Outcome Measures:Admission FIM scores, discharge FIM scores, length of stay (LOS), FIM gain, Length of Stay Efficiency (FIM Gain divided by LOS). Results:The morbidly obese (MO) group had an Admit FIM Score of 66.8 and a FIM Gain of 17.96. The non-obese (control) population had an Admit FIM Score 64.02 and a FIM Gain 17.90. The MO group had an average LOS of 17 days and a LOS Efficiency of 1.08. The control group had an average LOS of 14 days and a LOS Efficiency of 1.25. Statistical analysis showed a significant difference in LOS (p =0.025) but no significant difference in FIM Gain. Discussion:In this retrospective cohort study, morbidly obese patients had comparable admit FIMs and achieved comparable FIM gains over a longer period of time than non-obese patients. This is likely due to the increase difficulty with FIMs requiring mobility of the entire body. In subgroup FIM analysis, morbidly obese rehab patients had lower average admit scores in locomotion, transfers, stairs, lower body dressing, toilet / tub transfers, bathing and toileting. With the exception of stairs and tub transfers, these areas also showed higher average FIM gains in the morbidly obese cohort. These FIM gains in mobility contributed to a comparable rate of discharges to home but requiring longer lengths of stays. Morbid obesity is associated with many other medical conditions such as diabetes, which may have contributed to the higher rate of return to acute hospitalization in the obese population. Non-Obese Discharge Destination N=5384 Morbidly Obese Dischage Destination N=383 Examples of equipment used in our rehabilitation center: Barimaxx, KCI bariatric equipment, Arycare lift, Hoover mat and Stretch Bariatric chair (SIZEWise Rentals, L.L.C.) Conclusion:Morbidly obese rehabilitation patients required a greater length of stay to achieve FIM gains comparable to that of the non-morbidly-obese population. Activities requiring mobility of the entire body are of particular difficulty for the obese patient, but are also the areas of greatest potential gain. The morbidly obese rehab inpatients had a tendency to a greater rate of discharge to home, however, also had a greater rate of return to acute hospitalization as compared to the non-bariatric population. Barimaxx Bed (courtesy of KCI) Bariatric Equipment (courtesy of KCI) Arycare Lift (photo courtesy of AryCare) Hoover Mat and Stretch Bariatric Chair (photo courtesy of SIZEWise Rentals, L.L.C)