Download
1 / 37
370 likes | 379 Views
Protecting All Children’s Teeth. Special Needs. Introduction. Paper Permission on file from Joe Martinez.

E N D
Protecting All Children’s Teeth Special Needs www.aap.org/oralhealth/pact
Introduction Paper Permission on file from Joe Martinez • Approximately 18% of US children and youth have a special health care need. Many of these conditions, including mental retardation, developmental disabilities, cerebral palsy, craniofacial abnormalities, and seizure disorders, can impact a child’s oral health. By understanding the potential barriers to oral health care and the consequences of poor oral health in children with special health care needs, health professionals can identify at-risk patients early, provide anticipatory guidance, refer to appropriate dental professionals, and assist patients and families in overcoming barriers to accessing and utilizing care.
Learner Objectives Paper Permission on file from Joe Martinez • Upon completion of this presentation, participants will be able to: • Recall that dental care is the most common unmet need among the special needs population. • List barriers to accessing dental care • State reasons why children with special health care needs (SCHN) are at increased risk for caries. • Complete the oral health examination checklist at routine visits. • Assist families in addressing oral hygiene concerns and suggest techniques for optimizing oral care in children with special needs. • Discuss appropriate timing of referral to a pediatric dentist and list conditions that mandate early referral. www.aap.org/oralhealth/pact
Access to Care • For children with special health care needs, access to care may be limited. In the United States, dental care is the most common unmet need in the special needs population. Children with special needs are twice as likely than their aged-matched peers to not have their dental needs met.* • Families encounter greater difficulty obtaining needed dental care for children with certain diagnoses, including Down syndrome, other forms of mental retardation, cerebral palsy, and autism. www.aap.org/oralhealth/pact
Access to Care • Children with special health care needs may face the following barriers to accessing oral health care: • • Transportation or physical access to the building • • Financial strain, especially with multiple visits or costly restorative work • • Insurance coverage • • Difficulty finding a dentist who will see children with special health care needs • If a child has numerous medical concerns, families may consider oral health a lower priority.
Caries Risk • Children with special health care needs are at increased risk for developing caries for the following reasons:1. Diet • 2. Xerostomia • 3. Difficulties performing oral hygiene • 4. Gastroesophageal Reflux Disease and vomiting • 5. Gingival hyperplasia and crowding of the teeth • 6. Medications containing sugar www.aap.org/oralhealth/pact
Caries Risk, continued In children with special health care needs, uncoordinated chewing may leave more food in the mouth. A weak, uncoordinated tongue may not be able to adequately clean all oral surfaces. Gagging on the toothbrush, paste, or saliva may inhibit complete brushing of all surfaces. An inability to spit may result in the swallowing of toothpaste. www.aap.org/oralhealth/pact
Tooth Eruption • Tooth eruption may be delayed, • normal, or advanced in children • with special health care needs. Delayed eruption is more • common in children with Down • syndrome and hypothyroidism. Neonatal Tooth Eruption with Riga Fede Ulceration of the Tongue Used with permission from Martha Ann Keels, DDS, PhD; Division Head of Duke Pediatric Dentistry, Duke Children's Hospital www.aap.org/oralhealth/pact
Malocclusion and Crowded Teeth • Malocclusion and crowded teeth occur • more often in children with abnormal • muscle tone (cerebral palsy), mental • retardation, and craniofacial • abnormalities. Crowded teeth are more difficult to • clean, thereby increasing the risk of • dental caries and periodontal disease. Anterior Crossbite Used with permission from Martha Ann Keels, DDS, PhD; Division Head of Duke Pediatric Dentistry, Duke Children's Hospital www.aap.org/oralhealth/pact
Dental Anomalies • Teeth may vary in shape, size, or number. • Dental anomalies are a cosmetic concern and may increase the risk for caries. www.aap.org/oralhealth/pact
Gingival Hyperplasia • Gingival hyperplasia usually occurs • in children taking anti-epileptic • medications for seizures, especially • phenytoin. • Medications causing hyperplasia: • • Phenytoin • • Calcium channel blockers (nifedipine) • • Cyclosporin A • Chronic gingivitis from poor hygiene • can also trigger or exacerbate • medication induced gingival overgrowth. Used with permission from Rocio B. Quinonez, DMD, MS, MPH; Associate Professor Department of Pediatric Dentistry, School of Dentistry University of North Carolina www.aap.org/oralhealth/pact
Gingival Hyperplasia In addition to the cosmetic concern, gingival hyperplasia puts children at risk for: • Poor oral hygiene • Impaired tooth eruption • Difficulty chewing • Severe gingivitis Treatment includes:• Meticulous hygiene • Discontinuing the offending medication • Gingivectomy if severe www.aap.org/oralhealth/pact
Trauma • Trauma to the face and mouth • occurs more frequently in • children with seizures, • developmental delays, poor • muscle coordination, and • abnormal protective reflexes. Some children with special • needs exhibit self-injurious • behavior, which may damage • oral structures. Used with permission from Rocio B. Quinonez, DMD, MS, MPH; Associate Professor Department of Pediatric Dentistry, School of Dentistry University of North Carolina www.aap.org/oralhealth/pact
Bruxism • Bruxism is more common and often more severe in children • with cerebral palsy or severe mental retardation. • Bruxism may lead to enamel loss and difficulty with chewing or • tooth sensitivity. Children with suspected bruxism should be referred to a • pediatric dentist for evaluation. www.aap.org/oralhealth/pact
Problems With Oral Care • Children with special health care needs may not be able to • fully cooperate with oral hygiene practices due to gagging, • oral defensiveness, or behavioral issues They may also have difficulty tolerating fluoride liquid, • toothpaste, varnish, sealants, or other caries prevention • strategies www.aap.org/oralhealth/pact
Daily Preventive Care • Daily home preventive dental care may have to be tailored to meet the specific needs of the child • This is often best addressed by the dental and other health professionals involved in caring for the child • Patients with SHCN who have a dental home are more likely to receive appropriate preventive and routine care www.aap.org/oralhealth/pact
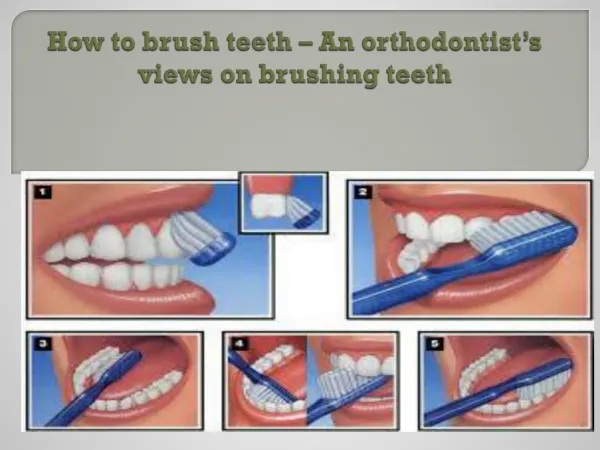
Toothbrushing • If there are concerns about swallowing toothpaste, families should minimize the amount of toothpaste used (a smear, less than a pea-sized amount) or use a non-fluoridated toothpaste. Used with permission from Guisy Romano-CLarke If gagging is triggered by toothpaste, the teeth can be brushed with fluoride mouthrinse. www.aap.org/oralhealth/pact
Toothpaste Amounts “Smear” “Pea-sized”
Toothbrushing • For older patients with limited dexterity, consider the following options: • An electric or battery-powered toothbrush • Extending the brush handle with a tongue depressor • Widening the brush handle (wrapping it with a sponge) • Using a mouth prop for brushing www.aap.org/oralhealth/pact
Dental Office • Children with special health care needs may require sedation even for routine cleanings, restorative procedures, and minimal oral surgery. If there is concern about a child’s cooperation or ability to tolerate oral manipulation, consider referral to a pediatric dentist or a specialist with training in sedation. Paper Permission on file from Joanna Douglass, BDS, DDS www.aap.org/oralhealth/pact
Pediatric Office Screening • Oral examination may be more difficult in a child with special health care needs. The primary care physician should make increased efforts to complete an examination checklist. Early referral to a dental professional comfortable treating children with SHCN (typically a pediatric dentist) will help ensure the oral examination is complete and all issues are addressed. Paper Permission on file from Mayra Patino www.aap.org/oralhealth/pact
Examination Checklist • The oral examination of a child with special needs is • similar to the routine child oral examination. Oral defensiveness, increased gag reflex, and oral • motor hypotonicity may make the examination more • difficult and should be documented. www.aap.org/oralhealth/pact
Examination Checklist, continued • Practitioners should examine • the following areas and • document abnormalities: • Oral-facial anomalies • Teeth • Gingiva • Palate Cleft Lip Used with permission from David A. Clark, MD; Chairman and Professor of Pediatrics at Albany Medical Center www.aap.org/oralhealth/pact
Referrals • All children with special health care needs fall into a high risk • category and should be referred to a dentist by 1 year of age. • Any child with evidence of caries or tooth, gingival, or eruption • anomalies should be immediately referred to a dentist who is • comfortable caring for children with special needs. www.aap.org/oralhealth/pact
Dental Insurance • Dental insurance coverage may be a problem for some • children who have special health care needs. Most of these children qualify for Medicaid, which automatically • qualifies them for comprehensive oral health services through • the Early and Periodic Screening and Diagnostic and Treatment • (EPSDT) program. www.aap.org/oralhealth/pact
Question #1 • Which of the following is not a risk factor for caries in • children with special needs? • A. Bruxism • B. Gastroesophageal Reflux Disease. • C. Xerostomia from the use of certain medications. • D. A special diet that is often cariogenic. • E. Oral motor hypotonicity. www.aap.org/oralhealth/pact
Answer • Which of the following is not a risk factor for caries in • children with special needs? • A. Bruxism • B. Gastroesophageal Reflux Disease. • C. Xerostomia from the use of certain medications. • D. A special diet that is often cariogenic. • E. Oral motor hypotonicity. www.aap.org/oralhealth/pact
Question #2 • You inform the family of a child with special needs that • the presence of gingival hyperplasia may put the child • at risk for which of the following: • A. Premature tooth loss. • B. Severe gingivitis. • C. Increased likelihood of tooth-grinding. • D. Increased risk of tooth injury from oral trauma. • E. All of the above. www.aap.org/oralhealth/pact
Answer • You inform the family of a child with special needs that • the presence of gingival hyperplasia may put the child • at risk for which of the following: • A. Premature tooth loss. • B. Severe gingivitis. • C. Increased likelihood of tooth-grinding. • D. Increased risk of tooth injury from oral trauma. • E. All of the above. www.aap.org/oralhealth/pact
Question #3 • Which of the following methods will help to prevent • children with special needs from swallowing • toothpaste? • A. Using less than a pea-sized amount of toothpaste. • B. Brushing the teeth with plain water. • C. Using a non-fluoridated toothpaste. • D. Using an electric or battery-powered toothpaste for children with limited dexterity. • E. All of the above. www.aap.org/oralhealth/pact
Answer • Which of the following methods will help to prevent • children with special needs from swallowing • toothpaste? • A. Using less than a pea-sized amount of toothpaste. • B. Brushing the teeth with plain water. • C. Using a non-fluoridated toothpaste. • D. Using an electric or battery-powered toothpaste for children with limited dexterity. • E. All of the above. www.aap.org/oralhealth/pact
Question #4 • True or False? For a child with special health care • needs, early referral to a pediatric dentist will help to • ensure the oral examination is complete. • A. True • B. False www.aap.org/oralhealth/pact
Answer • True or False? For a child with special health care needs, • early referral to a pediatric dentist will help to ensure • the oral examination is complete. • A. True • B. False www.aap.org/oralhealth/pact
Question #5 • Based on the AAP risk group designations, by what age • should children with special health care needs be • referred to a dentist? • A. 6 months • B. 9 months • C. 12 months • D. 18 months • E. 24 months www.aap.org/oralhealth/pact
Answer • Based on the AAP risk group designations, by what age • should children with special health care needs be • referred to a dentist? • A. 6 months • B. 9 months • C.12 months • D. 18 months • E. 24 months www.aap.org/oralhealth/pact
References • American Academy of Pediatric Dentistry. Policy on dental home. Pediatr Dent. 2012;34(special issue):24-5. • American Academy of Pediatrics Policy Statement. Oral health Risk Assessment Timing and Establishment of the Dental Home. Pediatrics. 2003; 111(5): 1113-1116. Available online at: http://pediatrics.aappublications.org/content/111/5/1113. Accessed Nov 11th, 2013. • Barzel R, Holt K, Isman B et al. Special Care: An Oral Health Professional’s Guide to Serving Young Children with Special Health Care Needs. Available online at: www.mchoralhealth.org/SpecialCare. Accessed Nov 11th, 2013. • Casamassimo P, Seale S, Ruehs K. General dentists’ perceptions of educational and treatment issues affecting access to care for children with special health care needs. J Dent Educ. 2004; 68(1):23–28. • Guideline on Management of Dental Patients with Special Health Care Needs. American Academy of Pediatric Dentistry Clinical Guidelines, Council on Clinical Affairs; 2012, Pediatr Dent; 35(6): 157-162. Available online at: www.aapd.org/media/Policies_Guidelines/G_SHCN.pdf. Accessed Nov 11th, 2013. • Lewis CW. Dental Care and Children with Special Health Care Needs: A Population-Based Perspective. Academic pediatrics. 2009. 420- 426. • Lewis CW, Robertson AS, Phelps S. Unmet dental care needs among children with special health care needs: implications for the medical home. Pediatrics, 2005. 116: e426–e431 www.aap.org/oralhealth/pact
References, continued • McPherson M, Arango P, Fox H et al. Commentary: A New Definition of Children With Special Health Care Needs. Pediatrics. 1998; 102(1): 137 –139. • Newacheck PW, McManus M, Fox HB et al. Access to Health Care for Children With Special Health Care Needs. Pediatrics. 2000; 105(4):760-766. • Newacheck PW, Strickland B, Shonkoff JP, et al. An Epidemiologic Profile of Children With Special Health Care Needs. Pediatrics. 1998; 102(1):117-121. • Perlman SP, Friedman C, Kaufhold GH. Special Smiles: A Guide to Good Oral Health for Persons with Special Needs. Available online at: http://media.specialolympics.org/soi/files/healthy-athletes/Special%20_Smiles_Good_Oral_Health_Guide.pdf. Accessed Nov 11th, 2013. • van Dyck PC, Kogan MD, McPherson MG et al. Prevalence and Characteristics of Children with Special Health Care Needs. Arch Pediatric Adolesc Med. 2004; 158(9): 884-890. www.aap.org/oralhealth/pact