Download
1 / 20
220 likes | 402 Views
Comparison of Umbilical Venous and Intraosseous Access During Simulated Neonatal Resuscitation. Anand Rajani, M.D. Perinatal Medical Group, Inc. Fresno, California Previous affiliation: Fellow in Neonatal-Perinatal Medicine Stanford University School of Medicine

E N D
Comparison of Umbilical Venous and Intraosseous Access During Simulated Neonatal Resuscitation • Anand Rajani, M.D. • Perinatal Medical Group, Inc. • Fresno, California • Previous affiliation: • Fellow in Neonatal-Perinatal Medicine • Stanford University School of Medicine • Lucile Packard Children’s Hospital • Palo Alto, California
Disclosure • I have nothing to disclose. • This work was supported by the Young Investigator Award from the Neonatal Resuscitation Program.
Background • While 10% of newborns require some assistance to begin breathing, only 1% require extensive resuscitative efforts • Less than 2 in 1000 births require administration of intravenous epinephrine1 • Proficiency in rapid umbilical venous catheter (UVC) placement is difficult to maintain 1. Perlman JM, Risser R. Cardiopulmonary resuscitation in the delivery room. Arch Pediatr Adolesc Med 1995;149:20 – 5
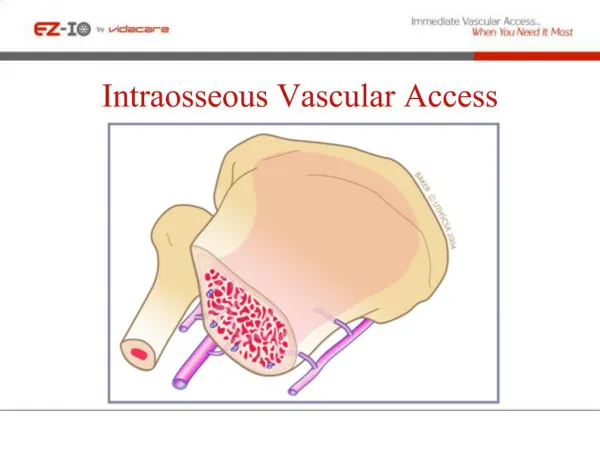
Background • Establishing umbilical venous access is frequently difficult • Catheter setup • Thoracic compressions • Moving sterile field • Data indicate that intraosseous needle (IO) placement is a safe and effective alternative • Access times of 30-60 seconds in the pediatric setting2 • Pharmacokinetic data on IO epinephrine in newborn lambs suggest equal efficacy3 • 2. Zaritsky AL, Nadkarni UM, Hickey RW, et al. PALS provider manual. Dallas (TX)7 AmericanHeart Association/American Academy of Pediatrics; 2002 • 3. Ellemunter H, Simma B, Trawoger R, et al. Intraosseous lines in preterm and full term neonates. Arch Dis Child Fetal Neonatal Ed 1990;80:F74-5.
Simulation • Allows for the re-creation of high-risk, low frequency events in numbers that are useful for statistical analysis • Can be video-recorded for further analysis • No harm to real patients
Hypotheses • Primary Null Hypothesis: • Ho: IO and UVC placement will be established in equal time • Secondary Null Hypothesis: • Ho: IO and UVC placement will be established with equal rates of error • Observational Null Hypothesis: • Ho: Perceived ease of use will be equal for UVC and IO
Methods • Recruited 40 healthcare practitioners of varying training levels from Lucile Packard Children’s Hospital at Stanford
Methods • Two standardized, videotaped simulated resuscitation scenarios in which intravascular access was indicated • A nurse and RT confederate performed CPR while the participant established access • Indistinguishable kits containing UVCs or IOs were available at the bedside • Simulation was stopped once access established
Methods: Study Design • Prospective, blinded, randomized, 2x2 crossover design • Randomized participants in separate blocks, by training level to perform either: • UVC/IO or IO/UVC • Prior to the simulations, participants watched a video reviewing the necessary steps involved in placement of a UVC and IO needle
Methods: Data Collection • Using video recordings: • Placement Time • Errors during placement • 4 error categories were used for each modality: • Site preparation • Device Preparation • Location and depth • Confirmation of access
Methods: Data Collection • Using questionnaire: • Users perception of technical difficulty (Likert scale from 0-10) • Preference for IO or UVC, if any • asked for reasons behind preference • space left for additional comments
Analyses for Primary Hypothesis • Ho: IO and UVC will be established in equal time • Test 1: t-test to evaluate for ‘period effect’ • Evaluate the difference in the two time periods of UVC/IO and IO/UVC • There was no significant difference in placement times for UVC or IO relative to placement order
Analyses for Primary Hypothesis • Test 2: Matched pairs t-test to evaluate for any difference in placement time between UVC and IO • For placement time, IO was significantly faster (p<0.0001) • Using ANOVAs, resident group was significantly faster than all other groups
Analyses for Secondary Hypotheses • Ho: IO and UVC will be established with equal rates of error • No significant difference was found • 3 errors in the IO group (site prep) • 1 error in the UVC group (site prep)
Analysis of Observational Hypothesis • Ho: Perceived ease of use will be similar for UVC and IO • UVC and IO found to be equivalent • Residents (n=16) found IO to be easier to place than UVC (p=0.003) • 25% (4) residents preferred IO; 2 had no preference • 22 participants preferred the UVC -- all cited familiarity as a reason for this preference • difference in experience: years vs. minutes!
Discussion • Difference between mean IO and UVC placement was 0.76 minutes (~46 seconds) • Identifies differences in time to placement -- does not account for how components are packaged • Implications for NRP / Possible practice changes • perhaps IO should also be taught and recommended as a placement technique (not shown to be inferior) • UVCs could be recommended for use in tertiary care centers where there is consistent experience; IOs may be more appropriate elsewhere
Conclusions • For the primary hypothesis: must reject Ho • IO is faster than UVC • For the secondary hypothesis: must accept Ho • no difference in rates of error • For the observational hypothesis: must accept Ho • no difference in perceived ease of use
References • Perlman JM, Risser R. Cardiopulmonary resuscitation in the delivery room. Arch Pediatr Adolesc Med 1995;149:20-5. • Zaritsky AL, Nadkarni UM, Hickey RW, et al. PALS provider manual. Dallas (TX)7 AmericanHeart Association/American Academy of Pediatrics; 2002 • Ellemunter H, Simma B, Trawoger R, et al. Intraosseous lines in preterm and full term neonates. Arch Dis Child Fetal Neonatal Ed 1990;80:F74-5. • Sapien R, Stein H, Padbury JF, Thio S, Hodge D. Intraosseous versus intravenous epinephrine infusions in lambs: Pharmacokinetics and pharmacodynamics. Ped Emerg Care 1992;8:179-183.