Download

1 / 24

E N D
الاجتماع الوزاري لغربي آسيا بمشاركة المجلس الاقتصادي والاجتماعي التابع للأمم المتحدة، ولجنة الأمم المتحدة الاقتصادية والاجتماعية لغربي آسيا، ومنظمة الصحة العالمية "التصدِّي للأمراض غير السارية وللإصابات: تحدِّيات كبرى تواجه التنمية المستدامة في القرن الحاديوالعشرين"تستضيفه دولة قطر في الدوحة، 10 – 11 أيار/مايو2009 ECOSOC/UNESCWA/WHO Western Asia Ministerial Meeting “Addressing noncommunicable diseases and injuries: major challenges to sustainable development in the 21st century” (Hosted by the Government of Qatar in Doha, 10-11 May 2009) Dr Douglas Bettcher, Director, TFI, WHO
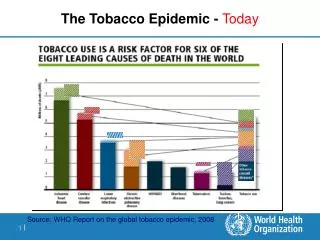
The Tobacco Epidemic Worsening... Unless We Act Now Smoking killed 0.1billion for 20th Century,but for the 21st century,SMOKING WILL KILL A TOTAL OF 1 BILLION (half the deaths in middle age). Tobacco currently kills:5 million/yr Will increase to: 8.3 million/yr by 2030.
The Leading Preventable Cause of Death in the World Source: WHO 2008
Foundation stone in the global fight against the tobacco epidemic. First global health treaty negotiated under auspices of WHO – adopted in 2003. Entry into force -27 Feb 2005. 164 parties as of 2009. WHO Framework Convention on Tobacco Control (WHO FCTC)
Status of the WHO FCTC in the region SYRIAN ARAB REP. TUNISIA ISL. REP. OF IRAN LEBANON AFGHANISTAN IRAQ oPt MOROCCO JORDAN PAKISTAN LIBYAN ARAB JAMAHIRYA EGYPT KUWAIT QUATAR UAE BAHRAIN OMAN SAUDI ARABIA CONTRACTING PARTIES to THE WHO FCTC SUDAN YEMEN COUNTRIES NON PARTIES THAT HAVE SIGNED THE WHO FCTC COUNTRIES THAT HAVE NOT SIGNED THE WHO FCTC AND ARE NOT CONTRACTING PARTIES SOMALIA
mpower: Six policies for tobacco control as part of WHO FCTC comprehensive implementation. Key entry point for scaling up tobacco control. Help countries build on WHO FCTC commitments. Integral part of the WHO Action Plan for the Prevention and Control of Non-Communicable Diseases. Matches WHO public health competency. Global Level Implementation of WHO FCTC – Country-level
TFI : Bringing in Change • monitor tobacco use and prevention policies • protect people from tobacco smoke • offer help to quit tobacco use • warn about the dangers of tobacco • enforce bans on tobacco advertising, promotion and sponsorship • raise taxes on tobacco
WHO FCTC and MPOWER An evidence-based tool for tobacco control (demand and supply side measures) r p w Article 6, 15 Article 8 Article 11, 12 e o m Article 13 Article 14 Article 20, 21
Tobacco use prevalence is higher among the poor Smoking prevalence in selected EMRO countries Source: World Health Survey 2006 Note: Q1-Q5: Lowest-Highest income groups
Tobacco control is good for developmentand for addressing social determinants of health • A recent study looking at systematic reviews to assess the impact of population-level tobacco control policies on social inequalities in smoking showed that: there was preliminary evidence thatincreases in the price of tobacco may have the potential to reduce smoking related health inequalities.
Tobacco control is good for developmentand for addressing social determinants of health • With regards to taxation,poor groups respond more to price increases and reduce tobacco consumption to a greater extent than other groups do.
Tobacco control is good for developmentand for addressing social determinants of health • Earmarking tobacco taxes – a pro-poor policy: Dedicating part (or all) of the revenues from tobacco taxes to develop NCD/health measures aiming at reaching vulnerable and poor populations is feasible and can render those measures more effective in reducing the burden of NCDs while at the same being pro-poor. • At the time of financial crisis, tobacco tax increase is a good way to generate revenue.
Earmarking tobacco taxes: examples from EMRO • Egypt: 10 piasters per 20 cigarettes are devoted to the students health insurance. • Qatar: 2% of revenues from import duties on tobacco products allocated for health awareness activities and tobacco control activities. • Jordan: 20 Flus (1/1000 of Jordanian Dinar) National Fund to support youth movement. • Tunisia: Rate varying by tobacco product between 10 and 170 millimes (millime=1/1000 Tunisian Dinar) per tobacco product to the activities of the Solidarity National Fund. • Iraq: 5% of imported value of cigarettes for reconstruction activities.
Earmarking tobacco taxes, a pro-poor policy Success story: Thailand • Health Promotion Foundation (ThaiHealth) set up in 2001 by the Government. • Receiving 2% of the total revenuesfrom alcohol and tobacco (about 35million$ per year). • Acts as a catalyst and supports groups and organizations already working on public health. • Inspired neighbouring countries: Mongolia adopted the same structure and received technical assistance from ThaiHealth in the process of setting up the policy.
Applying best practices in all countries Capacity building Economics Surveillance Legal Advocacy and Communications National tobacco control plans Country-level partnerships Global networks and partnerships TFI works with countries for building managerial, technical and policy infrastructure.
Applying best practices in all countries • Capacity Building- assessment of national capacity and support for policy development. • Monitoring and Evaluation– strengthen population based comparable surveillance (e.g. GATS). • Economics - technical support for economic research and interventions. • Advocacy and Communications- promote effective policies with partners using global and country media.
Trade unions Health Professionals Media NGOs PUBLIC AWARENESS JHBSPH CDC WLF IARC Bloomberg Philanthropies Working together to curb the tobacco epidemic WHO Collaborating Centres INTERNATIONAL SUPPORT SCIENTIFIC EVIDENCE Gates foundation Researchers Donor countries WHO Head quarter (TFI) Ministry of Health WHO Framework Convention on Tobacco Control Ministry of Agriculture Ministry of Finance INTERGOVERNMENTAL WORK Ministry of Justice Ministry of Education WHO Regional Office WHO Country offices POLITICAL WILL UN task force
Knowing is not enough; we must apply. Willing is not enough; we must do. Johann Wolfgang von Goethe (1749–1832) Thank you for your attention!
Mpower (supporting Article 20 & 21) Policy impact of country work • Egypt: Currently half way through GATS data collection. GATS national level data release is planned for September 2009. • Turkey: Launch of Turkish-language translation of the WHO Report on the Global Tobacco Epidemic - 2008 sparked considerable media attention. In 2009 - launch of the first GATS set analysed data.
mPower (supporting Article 8) Policy Impact of country work • Egypt : The2007 tobacco control law declared all public places to be free of tobacco, and was implemented except for restaurants and cafes. Similarly examples in Jordan, Bahrain and UAE. • SA: The only two tobacco free cities in the region. • Ireland: Adopted and implemented the first comprehensive smoke free law in 2004, changing the face of the smoke free policies in the 21st century.
mpOwer (supporting Article 14) Policy Impact of country work • Iran - Lots of work on cessation training - national training of trainers workshop on cessation, over 100 cessation centers set up. An area that needs further advancing in the region. • Nepal: Incorporation of brief cessation advice into PHC for chronic respiratory diseases and tuberculosis (2007- June 2008).
Jordan isfirst country to have pictorial health warnings(30%); Egypt is first country to have 50% of the pack size, followed by Iran, Djibouti. All GCC countries are in process of selecting their pictorial health warnings. Australia: Strong picture health warnings on both covers front (30%) and back (90%). Policy Impact of country work mpoWer(supporting Article 11 & 12)
mpowEr(supporting Article 13) Policy Impact of country work • Total ban on advertising exists and is implemented in 9 MS of EMRO: Djibouti, IRAN, Jordan, Kuwait, Qatar, Sudan, UAE, Yemen, EGY. • Thailand: In addition to ban of advertisement, product display at point-of-sale is banned.
mpoweR(supporting Article 6) Policy Impact of country work • Thailand: A high percentage of the price of a pack of cigarettes goes to taxes in Thailand (64%), and 2% of total revenues from tobacco and alcohol are used for health promotion.