Download
1 / 6
360 likes | 1.5k Views
Physiology of the Esophagus. Dr. JH Barnard Dept. of Surgery PAH 19/03/2002. Introduction:. The gastrointestinal tract is devided into different compartments.

E N D
Physiology of the Esophagus Dr. JH Barnard Dept. of Surgery PAH 19/03/2002
Introduction: • The gastrointestinal tract is devided into different compartments. • Every compartment can be regarded as consisting of a pump, a sphincter and a reservoir.The pharynx being the pump, the upper esophageal sphincter (UES) the valve upper esophagus (reservoir). The same can be said for lower esophagus, the LES and stomach. • Not one directional valves, in health this backflow is limited.
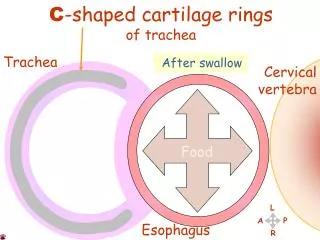
Pharingoesophageal Segment: • During swallowing the tongue, pharynx acts as a pump; soft palate, epiglottis, UES functions as three valves. Failure of either leads to problems in the swallowing mechanism. • Immobility of the tongue due to radiation or chemical burns and paresis may also lead to disphagia. • The hyoid bone moves up and anterior, opening the retro pharyngeal space. • Pressure 60mmHg. Duration 1,5s
Esophageal Body: • Pressure gradient over UES accentuated because intra-thoracic pressure is negative • From mid esophagus a pressure gradient must be overcome PERISTALSIS • Pressure 30-120mmHg • Amplitude increases from mid-esophagus to cardia • Travels at 2-4 cm/s. 7s to stomach. 20 cm/s regarded as simultaneous wave
Peristalsis:cont. • To be effective must be both sufficiently organized and of good amplitude • Clinically peristaltic defects can be divided into two broad categories: A)Defect in organization, neural phenomenon B) Reduction in power, muscle damage because of reflux or scleroderma
Lower Esophageal Sphincter • Pressure barrier between esophagus and stomach. • Relaxes shortly after swallow (incomplete=achalasia) • LES must prevent reflux from the positive intra abdominal to the negative intra thoracic pressure. Effectiveness depends on the resting pressure of the LES, abdominal length of the esophagus, overall length of the esophagus.