Download
1 / 91
1.01k likes | 1.3k Views
MRI Shoulder Joint. Dr. Anand M Rahalkar MD, DNB. Introduction. Extremely useful modality. Only modality which can assess the labrum with minimal invasion. Easily available, no radiation.

E N D
MRI Shoulder Joint Dr. Anand M Rahalkar MD, DNB
Introduction • Extremely useful modality. • Only modality which can assess the labrum with minimal invasion. • Easily available, no radiation. • Clearly scores over X-ray, CT arthrography & USG for depiction of the anatomy. USG is useful only for rotator cuff tears, impingement and evaluation of humerus.
Positioning • Shoulder and arm are placed in neutral position / external position. • Full rotation is difficult and can lead to motion artifacts. Also the biceps is not clearly seen. • In internal rotation anterior capsular structures appear more lax & less sharply defined. • Neutral position– thumbs up position of the extended hand.
Protocol • T1 axial localizer to see the SST tendon. • Cor Oblq. & Sag Oblq. images are planned parallel & at right angles to the tendon. Direct coronal can give false impression of a tear. • Cor Oblq. T1 & fat sat PD T2/ STIR images. • Sag Oblq. T1 & fat sat PD T2/ STIR. • Ax Gr. T2 for the labrum. • MR arthrography. with ABER protocol to evaluate anterior instability. • T2 : short ETL to reduce image blurring & long TE.
Protocol • 3-4 mm thickness. • 256 x 256/129 matrix. • TE : 40-50 msec. • FOV : 10-14cm. • Cor oblq & Sag oblq sequences.
MR Arthrography • MR arthrography is to diff b/w partial & full thickness tears & for labral evaluation. • Technique: 0.2 cc Gad in 20 cc of saline & 5cc of nonionic contrast. 12-16 cc is injected under fluoroscopy. • MR imaging should be started within 30 min. of the procedure so that there is no contrast absorption and loss of capsular distention. • T1 fat suppressed images are obtained in all 3 planes and a T2 fat sat sequence for detecting labral cysts, and bone marrow lesions.
MR arthro • Pitfalls : extra-articular injection of contrast can spread along fascial planes in the SA-SD space which can be mistaken for a full thickness rotator cuff tear. • To avoid injection into the subscap tendon or IGL a posterior approach may be used. • Inadvertent injection of gas mat lead to false diagnosis of intra-articular loose bodies. However, loose bodies are dependent & gas is nondependent.
Anatomy • Osseous: articular surface of the glenoid & humerus. The bony glenoid is deepened by the labrum which is formed by the fibrous attachment of the GHL & capsule to the glenoid rim. It provides an area of attachment for the GHL. • The attachment of the sup labrum is more variable above the epiphyseal line i.e. the junction of the upper & middle 1/3rd of the glenoid. • The glenohumeral lig are the thickenend bands of the anterior joint capsule.
Con’td IGL has ant & post bands forming axillary pouch & contributes to the formation of the labrum. MGL is more variable in size & thickness & runs b/w the subscap tendon & ant band of IGL. It attaches to the neck of the humerus & the lesser tuberosity. SGL is smallest. Attaches to the upper pole of the glenoid & base of the coracoid process. Other ligaments: coracohumeral & coracoacromial- is the key structure in impingement disorders, attaches to the lat aspect of the coracoid & the acromion. The acromial attachment of the ligament can give a pseudospur appearance.
The superior labrum functions in conjunction with the biceps tendon . • 3 types of BLC are described acc to attachment. 1) firmly attached with no foramen. 2) Biceps attaches lat to the sup glenoid & leaves a sublabral sulcus. 3) Meniscoid labrum with a large sulcus. ACROMION: 4 types acc to shape (X-ray/MRI) 1) flat/straight inferior surface. 2) curved smooth inf surface parallel to humerus. 3) has ant. inf. hook-80% asso with impingement. 4) undersurface which is convex near its distal end. .
TYPE I TYPE II TYPE III
Acc to slope is either anterior/ lateral down sloping. • Anterior down sloping acromion has the anterior inferior cortex more inferiorly located relative to the post cortex on sag oblq images. Increases risk for anterior acromial impingement. • Lateral down sloping narrows the acromiohumeral distance, best seen on cor oblq images. Inferior surface of the distal acromion is more inferiorly placed as compared to its prox aspect. It increases incidence of impingement of SST near its insertion on the gr tub. • Other acromial variations include os acromiale which is unfused ossification centre.
Lat down sloping Acromion slope
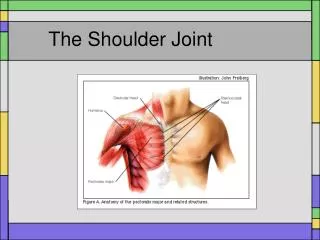
Muscles & bursae • Rotator cuff: SST, IST, Teres minor muscles insert on to the greater tuberosity. The subscap inserts on the lesser tuberosity. Together stabilise the GHJ. • The long head of biceps is intracapsular & originates from the supraglenoid tubercle. It runs in the bicipital groove & contributes to the labrum. • Bursae : SA-SD: extends under the acromion & coracoacromial lig . It lies over the sup. surface of the SST & IST. Does not normally commu with the GH joint & subscap bursa. The subscap & subcoracoid recesses & biceps tendon sheath communicate with the GHJ.
Shoulder impingement • Degenerative changes in the rotator cuff (SST) near the attachment to the gr tub. Commonest location is b/w the ant 1/3 of the acromion & the underlying tendon. • Aetiology :1) hypovascularity of the tendon • 2) mehanical wear, trauma • 3) acromial spurs, shape & slope • 4) AC joint morphology • 5) loss of humeral head depressors-rot cuff tears, biceps tendon rupture, trapezius palsy, chronic SA bursitis.
No impingement SST impingement
Rotator cuff tears • SST tears are most common as a result of impingement. • Can be either complete(AP) or incomplete. FULL THICKNESS PARTIAL FULL THICKNESS (SI) BURSAL ARTICULAR
Signs of tear Tear is defined as T2W hyperintensity. Magic angle effects are seen on low TE images(T1 & PD) at 55deg & should not be mistaken for tear. Tendinosis produces increased signal on T1& PD with thickening of the tendon. • Full thickness : • 1) non-visualisation of the tendon. • 2) retracted tendon/ fatty atrophy with time. • 3) gap in the tendon. • Sec. Signs : • 1)Fluid in the SA bursa. • Partial thickness: hyperintensity on T2W image on the bursal/articular surface.
Full thickness incomplete tear
Articular surface tear
Subscap tear
ROTATOR TEAR NORMAL
BEWARE OF MAGIC ANGLE ON SHORT TE
GHJ instability • Anterior instability : most common, produced by lesions of the IGLLC. • 1) Bankart’s lesion. • 2) ALPSA lesion. • 3) GLAD lesion. • 4) HAGL lesion.
Bankart’s lesion • It represents either the anterior labral avulsion or labral & anterior inferior glenoid fracture with displacement. Perthes is non-displaced labral detachment. Both have stripping of scapular periosteum. • Ax T1/ T2 GR are very useful for evaluation. Cor & Sag Oblq are useful to know the extent. • Acute lesions show increased signal intensity in the subchondral bone. A Hill Sach’s posterolateral compression can be seen with a single/ multiple episodes of dislocation. It is typically seen at or above the coracoid. Below is a normal groove of the humeral head.
Bankarts lesion Perthes lesion