Download
1 / 27
680 likes | 2.05k Views
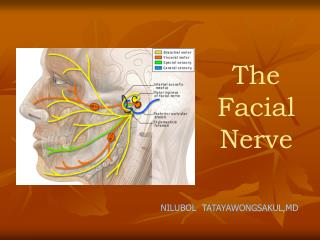
Facial Nerve. Bastaninejad Shahin , MD, Otolaryngologist. VII th nerve Anatomy. 4mm. 11mm. 8-10 IAC. 15-17 CPA. 13mm. Porus Fundus. G.G. Selected Clinical Scenarios. Bell’s Palsy. Spontaneous idiopathic facial paralysis

E N D
Facial Nerve BastaninejadShahin, MD, Otolaryngologist
4mm 11mm 8-10 IAC 15-17 CPA 13mm PorusFundus
Bell’s Palsy • Spontaneous idiopathic facial paralysis • paralysis or paresis of all muscle groups of one side of the face • sudden onset • absence of signs of CNS disease • absence of signs of ear or cerebellopontine angle disease
Incidence 20-30/100000, it’s greater in more than 65yrs • M/F ratio is equal, but in less than 20yrs it’s more common in F; but in more than 40yrs, it’s more common in M. • 30% have incomplete paralysis • 70% have complete paralysis
Bell’s Etiology • Microcirculatory failure of vasanervorum • Viral infection most accepted concept • Ischemic neuropathy • A.I. reaction HSV Reactivation
Other caranial nerve involvment in Bell’s palsy (in more than 50% of the pts): 5,7,9,10 + C2
Site of involvement: proximal Labyrinthine and meatal portion • Prognosis is excellent: 80-90% complete recovery (95-100% in partial paralysis) • Poor outcome measures: • Hyperacusis (brain stem reactivation) • Decreased tearing • Age more than 60 • DM and HTN • Severe aural and facial radicular pain
Bell’s Palsy (cont’) • Bell’s in Children • Female preponderance • 97% full recovery • Impact of corticosteroid is uncertain! • Familial Bell’s8% • Recurrent9.3% • More common in females, and DM sufferers • No prognostic difference with primary Bell’s
Bell’s in pregnancy • More frequent in pregnant women (*3.3) • Most common in third trimester or immediate postpartum • Pre-eclampsia is a RF • Treatment is with prednisolone
Management: • Corticosteroids (mainstay) : 1mg/kg/day in seven days, then taper it down • Antiviral agents • Surgery: within 2wks if ENOG showed more than 90% axonal degeneration (Gantz et al.)
Ramsay Hunt Syndrome (RHS) • Skin vesicles (aural, facial ,...) + faicial nerve paralysis • Relates to VZV ( while Bell’s was HSV ) • It’s 2nd most common cause of the facial paralysis • Complete recovery: • In complete paralysis 10%! • In incomplete paralysis 66% Poor outcome
Treatment is with Corticosteroid and Acyclovir • The main benefit of the corticostroid is reduction of postherpetic neuralgia, vertigo and acute pain ( it’s usefulness on recovery of the nerve is controvercial)
Congenital facial paralysis • Birth trauma 78% • Syndromic (Mobius syn., CHARGE,...) • Surgical exploration and decompression of the nerve is rarely useful • Main option is muscle transfer. 6th and Mastoid segment of the 7th nerve
Bilateral Facial Paralysis • Guillain barre syndrome (9, 10, 7) • Bell’s palsy 0.3 to 2% of pts • Idiopathic cranial neuropathies • Brain stem encephalitis • BIH • Syphilis • Leukemia • Sarcoidosis, Lyme disease &...
Traumatic Facial Paralysis • Most susceptible region: distal Labyrinthine and Geniculate ganglion • Surgical timing depends on the onset after injury (late, immediate)
Blunt head truma (sharp nerve cut repair in 3 days) • Surgical time planing: • Immediate paralysis: 3 wks after onset • Delayed paralysis: Expectant management and corticosteroids will be Okay!, but surgery indicates when you see gross disruption of fallopian canal in the CT-scan. • Fisch advocates surgical intervention on the basis of ENOG, rather than time of onset of the paralysis (...>90% degeneration within 6 days of onset)
Otitis Media • AOM, COM, Cholesteatoma • Most susceptible segment is Tympanic part • AOMIV Abx + Myringotomy • Cholesteatoma Removal of the choles. + nerve decompression without opening the perineurium • COM decide regarding to the degree of inflammation