Download
1 / 15
200 likes | 1.1k Views
Developed because of the increasing resistance of staphylococci to natural penicillins Alexander Fleming: Discover Penicillin on September 15, 1928

E N D
1.
Penicillinase-resistant Penicillins
Presented by
Abdulaziz M. Al - Saad
2. Developed because of the increasing resistance of staphylococci to natural penicillins
Alexander Fleming: Discover Penicillin on September 15, 1928
Resistance
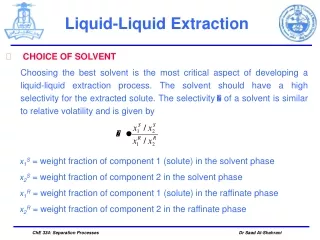
3. They are B-lactam acetylated with ( Bulky group ) , which give protection against ( penicillinase enz. ) by providing steric hindrance . They are fit into 3 chemical groups :
1- Phenyl Penicillins : 2- Isoxazoyl Penicillins :
3- Naphthyl Penicillin :
4.
Treatment of infections such as :
Osteomyelitis , Septicemia , Endocarditis , pneumonia , skin and soft tissue infection , CNS infection caused by staphylococci species ( Penicillinase producing ) .
1- Staphylococci species
2- Staphylococcus aureus
3- Streptococcus pneumonia
4- Strep. Faecalis & viridance ( Nafcillin ) .
Note : Temocillin is effective against G �ve except pseudomonas aeruginosa.
- Nafcillin + Gentamycin ------ Endocarditis .
- Nafcillin + Rifampin --------- DOC for chronic staph. Osteomyelitis .
- Nafcillin ---------------------- More effective than vancomycin for MSSA .
Mechanism of action 2 :
Inhibit cell wall synthesis by binding to PBPs --- Inhibit final transpeptidation --- No peptidoglycan . First, I would like to present a case of a patient that will illustrate one route of seeding of bacteria into the bony tissue to produce osteomyelitis. First, I would like to present a case of a patient that will illustrate one route of seeding of bacteria into the bony tissue to produce osteomyelitis.
5. 1- Methicllin :
Not used in general therapy ------- ( Why ? ) .
Higher incidence of nephrotoxicity & hypersensitivity > other pen.
MRSA ( intrinsic resistance ) ----------- explain .
2- Nafcillin :
Higher activity than ( methicillin & isoxazoyl pen. ) against pneumococci & hemolytic strept. cocci .
Acid stable but not recommended orally ( why? ) .
3- Isoxazoyl penicillins ( oxa , diclo , clo , flu. ) :
Isoxazoyl group leads to -------- 1- Resistance to b- lactamase .
2- Resistance to gastic acid .
3- Effective anti-staphylococcal .
A. Oxacillin : Constricted for treatment of staph. Resistance to Pen G ( Why? ) .
B. Cloxacillin : - CL at ortho position ----- Enhance activity over Oxacillin ( Why? )
- More potent than Methicillin .
C. Dicloxacillin : - 2 CL at ortho position ------------ Enhance stability & activity
- More potent than Cloxacillin .
Another example of seeding of the bony tissue to produce osteomyelitis. This patient is more complex as he has a true allergy to penicillin involving rash and Steven-Johnson�s syndrome. Another example of seeding of the bony tissue to produce osteomyelitis. This patient is more complex as he has a true allergy to penicillin involving rash and Steven-Johnson�s syndrome.
6. Generally, Penicillin cause Hypersensetivity , GIT disturbance , Fever .
Methicllin :
Nephrotoxicity ( large IV dose ) >>> ( symp. & sign ) , treatment ?
Leukopenia : Decrease neutrophils & lymphocyte ( < 500/mm3)
Isoxazoylyl Pen. :
Hepatotoxicity : Rapid disappear after stop medication .
Neurotoxicty ( large IV dose ) : Especially in patient with RF .
Hematological : Neutopenia ( especially with Oxacillin 200mg /kg dailly) .
Note : flucloxacillin increase risk of juandice .
Naficillin :
Nephrotoxicity ( large IV dose ) .
Hypokalemia & alkalosis : ( why ? )
Hematological : Neutopenia , Platelet dysfunction ( abnormal bleeding time ) .
By definition, osteomyelitis is an infectious process of the bone(s). Rarely, more than one bone can be involved. A good example of this occurring is when a patient has diabetic foot infection and more than one bone in the foot is involved. Another example is if a patient has more than one vertebrate involved in a case of vertebral osteomyelitis.
Classification of the disease cam be based on the route of entry of organisms to the bone. Here, two methods of inoculating the bone are identified. First, contiguous spread of organisms can occur from things such as trauma, injury, etc. Second, patients can develop bacteremia and then the bone can become infected by hematogenous bacterial emboli lodging in the bone. By definition, osteomyelitis is an infectious process of the bone(s). Rarely, more than one bone can be involved. A good example of this occurring is when a patient has diabetic foot infection and more than one bone in the foot is involved. Another example is if a patient has more than one vertebrate involved in a case of vertebral osteomyelitis.
Classification of the disease cam be based on the route of entry of organisms to the bone. Here, two methods of inoculating the bone are identified. First, contiguous spread of organisms can occur from things such as trauma, injury, etc. Second, patients can develop bacteremia and then the bone can become infected by hematogenous bacterial emboli lodging in the bone.
7. Another method of describing osteomyeolitis is to divide the disease up into acute and chronic osteomyeolitis. I don�t believe that it matters how one determines the cause of the disease. However, chronic osteomyelitis is one in which a patient has failed acute osteomyelitis treatment and therefore, will need to be treated for a period of time that will be longer than acute osteomyelitis treatment.
Waldvogel surveyed his experience at Massachusetts General Hospital and found the following causes of osteomyelitis. Of interest is that there were 247 cases of osteomyelitis in a four year time period. This is approximately 5.1 cases/month. Therefore, osteomyelitis is not a very prevalent disease. However, it does lead to a lot of morbidity with significant economic consequences. Another method of describing osteomyeolitis is to divide the disease up into acute and chronic osteomyeolitis. I don�t believe that it matters how one determines the cause of the disease. However, chronic osteomyelitis is one in which a patient has failed acute osteomyelitis treatment and therefore, will need to be treated for a period of time that will be longer than acute osteomyelitis treatment.
Waldvogel surveyed his experience at Massachusetts General Hospital and found the following causes of osteomyelitis. Of interest is that there were 247 cases of osteomyelitis in a four year time period. This is approximately 5.1 cases/month. Therefore, osteomyelitis is not a very prevalent disease. However, it does lead to a lot of morbidity with significant economic consequences.
8. Not removed by hemodialysis
No dose reduction in renal impairment ( except sever cases ) ( oxa , cloxa, diclo, fluclo ) but methicillin need.
Naficillin : Dose reduction in liver dysfunction .
Drug-drug Interactions 2 :
Naficillin is strong inducer of CYP 3A4 , But Dicloxacillin is weak
B-lactam( penicillin ) + Aminoglycoside ------- Chemical incompatibility
Probenecid + Pen. ------------------------------------ Increase level of Pen.
3. Penicillins ------------------------------------- Increase exposure to Methotrexate
Chloramphenicol + Pen. --------------------- Decrease efficacy of naficillin .
Naficillin + Cyclosporin -------------------Subtherapeutic levl of cyclosporin .
Pregnancy 2 :
Pregnancy risk factor B .
Cross placenta
Enter breast milk ( Use with caution ) .
This slide depicts the anatomy of our long bones (ie femur). Here we can see that capillaries make hairpin turns at the metaphyseal area of the growth plates. This is where bacterial emboli will lodge in this small areas of the hairpin turns and produce an inflammatory reaction resulting in bony necrosis and more inflammation associated with the bacteria. Symptoms that the patient will display will include pain at the site of infection, and possibly fever and chills. This slide depicts the anatomy of our long bones (ie femur). Here we can see that capillaries make hairpin turns at the metaphyseal area of the growth plates. This is where bacterial emboli will lodge in this small areas of the hairpin turns and produce an inflammatory reaction resulting in bony necrosis and more inflammation associated with the bacteria. Symptoms that the patient will display will include pain at the site of infection, and possibly fever and chills.
9. Contraindications 2:
Hypersensitivity to Penicillin .
Elder people : Not treated with Methicillin , but use Naficillin .
Sodium content 3 :
Must be considered in patients on restricted Na+ intake ( e.g.. HTN ) .
Mode of administration 3 :
Dicloxacillin ( orally )
Oxacillin , Cloxacillin , Fluoxacillin ( Orally , Parentrally ) .
Methicillin & Temocillin ( Only inject able )
10. Of importance, is that for the most part, hematogenous osteomyelitis is primarily a disease of children. Here, children develop bacteremia and then the bones become involved after bacteria in the bloodstream attempt to escape phagocytosis and seed the bone. Of importance, is that for the most part, hematogenous osteomyelitis is primarily a disease of children. Here, children develop bacteremia and then the bones become involved after bacteria in the bloodstream attempt to escape phagocytosis and seed the bone.
11. Take all medication , don�t skip doses ,
Take it 1 hr befor or 2 hr after meals [ Enhance F ] .
Missed dose- take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not double doses.
Storage :
Keep out of the reach of children.
Store away from heat and direct light.
Do not store the capsule or tablet form of penicillins in the bathroom. Heat or moisture may cause the medicine to break down.
Store the oral liquid form of penicillins in the refrigerator because heat will cause this medicine to break down. However, keep the medicine from freezing. Follow the directions on the label.
Do not keep outdated medicine or medicine no longer needed. Be sure that any discarded medicine is out of the reach of children.
12.
1. Methicillin :
- Sensetive to moisture --- Loss � of its activity after 5 days at RT .
- Solution for parental ad. May kept for 24 hr ----- [ at 5oC ] .
2. Nafcillin , Oxacillin :
Parentral sol. Stable for 3 days at RT. ( 96 hr if ref. ) .
3. Dicloxcillin :
Parentral sol. Stable for 7 days at RT ( 14 day if ref. ).
4. Cloxacillin :
Parentral sol. Stable for 14 days ( ref. ) .
5- Flucloxacillin :
Parentral sol. Stable for 7 days ( ref. )
Storage :
Store between 15 � 30oC
13. References : Web site e.g. www. .com .
Drug Information Handbook 12th Edition 2004 � 2005 pages ( 452 , 642 , 1062 , 1137 ).
USP DI Edition 1999 , pages ( 2251, 2252, 2253, 2254, 2255, 2256, 2262 ) .
Principle of Medicinal Chemistry 4th Edition page 778-779 .
15. Temocillin is a beta-lactamase-stable penicillin with a selective. Gram-negative spectrum of activity and a long half-life The urinary excretion by 12 h was 70.58% of the administered