Download
1 / 29

E N D
Case Study 8 Craig Horbinski, M.D., Ph.D.
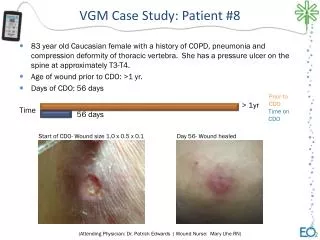
Question 1 Clinical history: 45-year-old white female with type I diabetes mellitus starting at age 13, complicated by diabetic neuropathy, gastroparesis, and end stage renal disease. She also had a history of retinal hemorrhages, retinal detachment, pulmonary embolism, schizophrenia, depression, hypertension, and gastrointestinal bleeding. She was a non-smoker, consumed no alcohol, and did not use illicit drugs. She had a long history of repeated renal transplantations and a pancreatic transplantation, all of which failed. Ultimately she died from a combination of end stage renal disease, atherosclerotic disease, and presumptive cardiac arrhythmia. An autopsy was performed.
Answer Ventriculomegaly and bilateral caudate nucleus atrophy
Question 2 Given the gross findings, what one thing was probably left out of the clinical history on page 1 (i.e. what one other disease did this woman likely have)?
Answer History of movement disorder, Huntington disease on the maternal side of her family (maternal grandmother, mother, aunt, and older brother).
Question 3 Describe what you see. Click here to view slide.
Answer Atrophic caudate nucleus, old lacunar infarct at the inferomedial caudate (note the macrophages the lacunar infarct is likely related to the patient s type 1 diabetes). Hard to do much else with this when it comes to evaluating for neurodegenerative diseases, the absence of neurons is harder to appreciate than the presence of something that s not supposed to be there.
Question 4 Normally chronic neuronal loss is identified by reactive astrocytosis, but in this case it s not readily apparent on H&E. What immunostain might help?
Answer GFAP
Question 5 Are there reactive astrocytes? Click here to view slide.
Answer Yes, but not a lot mostly around the medial (i.e. subventricular zone) and near the old lacunar infarct.
Question 6 Despite the patient s extensive family history of Huntington disease, she had refused testing while alive. What s the diagnostic molecular test for HD?
Answer PCR amplification of the CAG repeat region on chromosome 4 where the huntingtin gene is located. Normally it s done on fresh tissue (usually patient s blood), but it can be done on formalin-fixed, paraffin-embedded tissue.
Question 7 The PCR analysis showed alleles of ~20 and ~44 CAG (polyglutamine) repeats. Does this confirm HD?
Answer Yes. Individuals who do not have HD usually have 28 or fewer CAG repeats. Individuals with HD usually have 40 or more repeats. Some are within the borderline range of repeats, and may or may not exhibit symptoms. Because it is an autosomal dominant disease, only one allele need have expanded repeats.
Question 8 What is the main type of neuron lost in Huntington disease? What sort of movement disorder would you see intention tremors or resting tremors?
Answer Medium spiny GABAergic neurons in the caudate nucleus. Due to the loss of inhibitory feedback loops in the basal ganglia, the ability to fine-tune movements is lost and severe tremors manifest when the patient tries to move (intention tremors). Resting tremors are the hallmark of Parkinson disease, which involves the loss of substantia nigra neurons in the midbrain and, thus, disrupts an entirely different motor pathway (dopaminergic).
Question 9 What is the best additional stain to order that would further support these findings?
Answer Ubiquitin immunostain. Huntington disease is characterized microscopically by ubiquitin-positive intranuclear inclusions within the caudate nucleus and, later, in the putamen.
Question 10 Are there any ubiquitin-positive intranuclear inclusions? Click here to view slide.
Answer Yes many neurons in the caudate nucleus and putamen have ubiquitin-positive intranuclear inclusions. Nonspecific speckles in the white matter are also present.
Question 11 What phenomenon is commonly seen in multiple generations affected by trinucleotide repeat diseases? What causes this phenomenon?
Answer Anticipation, where the onset of disease occurs earlier, and the severity worsens, with each subsequent generation. It is widely held that the expanded trinucleotide repeats are physically slippery for the DNA polymerase during meiotic cell division, and the polymerase ends up adding a few more repeats during each generation of germ cell proliferation.
Question 12 This patient is the third generation afflicted with HD, yet she only has 40 polyglutamine repeats and survived 45 years (maybe longer if she hadn t had type 1 DM). How do you reconcile this with the well-known anticipation phenomenon?
Answer The anticipation effect in HD is best seen when the diseased gene is inherited through the paternal line. This patient s HD was inherited through the maternal line. Theories as to why this happens include some sort of imprinting or X-linked comodifier, the former being favored (Am J Hum Genet. 1995 Sep 57(3):593-602; Am J Hum Genet. 1992 Mar 50(3):536-43).
Question 13 Go back to the original gross image. What is the grading system used to describe the severity of HD? What is the grade in this case?
Answer Vonsattel grading system • Grade 0 no caudate atrophy seen grossly, no gliosis, 30-40% loss of neurons microscopically • Grade 1 no caudate atrophy seen grossly, moderate gliosis, 50% loss of neurons microscopically • Grade 2 grossly visible atrophy of head of caudate while retaining convexity • Grade 3 caudate head is a flat line, with noconvexity at all • Grade 4 caudate is concave This is a Vonsattel grade 2 of 4.











![Debating Stem Cells [Case Study 8]](https://cdn1.slideserve.com/2827886/debating-stem-cells-case-study-8-dt.jpg)