Download
1 / 84
1.02k likes | 1.94k Views
ACUTE ABDOMINAL PAIN. Victor Politi, M.D., FACP Medical Director, SVCMC School of Allied Health, Physician Assistant Program . Abdominal Pain. Most common cause of hospital admission in the US Accounts for 5-10% of all ED visits

E N D
ACUTE ABDOMINAL PAIN Victor Politi, M.D., FACP Medical Director, SVCMC School of Allied Health, Physician Assistant Program
Abdominal Pain • Most common cause of hospital admission in the US • Accounts for 5-10% of all ED visits • In 35-40% of all hospital admissions due to abdominal pain - the pain is nonspecific
Epidemiology • Gastroenteritis is the most common cause of abdominal pain not requiring surgery • In patients age 60 and older, biliary disease and intestinal obstruction are the most common cause of acute abdominal pain that is surgically correctable
Epidemiology • Appendicitis is the most common cause of abdominal pain requiring surgery in patients < age 60 • Appendicitis is the leading cause of acute abdominal pain in children • accounts for 32% of children admitted w/acute abdominal pain
Patient History • The term “acute abdomen” implies the sudden onset of abdominal pain for which a surgically correctable cause is likely
Patient History • Besides the age of the patient - key elements of the patient history include: • Time of pain onset • Location/character of pain • Pattern of pain radiation • Associated symptoms
Key Points in History • Reproductive • Sexual Activity, Contraception, Last Menstrual Period • Always Consider Pregnancy in Reproductive Age Women • Have a Low Threshold for Pregnancy Testing • Bowel and Bladder • Nausea, Vomiting, Diarrhea, Constipation • Frank Blood, "Coffee Grounds" Emesis, Black Stools • Urinary Frequency, Urgency, Discomfort
AGE • Age of patient - crucial • Differential diagnosis of abdominal pain in children - differs from dx in elderly patient • Common conditions that cause abdominal pain in most age groups • acute appendicitis, intestinal obstruction, incarcerated hernias
AGE • Intussusception is most likely the cause of intestinal obstruction in children • Adhesions are most likely the cause of intestinal obstruction in adults • In older patients, pain from a MI can be referred to the upper abdomen
Time of Onset • Pain sudden in onset, awakens a patient from sleep - suggests a viscus • Knowing the timing of associated nausea and vomiting is essential to narrow the diagnostic possibilities • Pain precedes vomiting when abdominal pain is from surgically correctable causes, whereas the reverse is true for medical conditions such as gastroenteritis
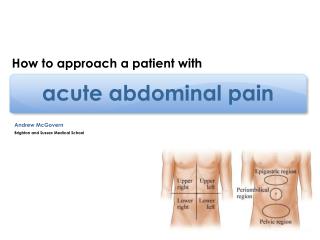
Location • Abdomen divided into 4 quadrants, which are further divided (with some overlap) into the epigastric, periumbilical, and suprapubic regions
Location of Abdominal Pain • Four quadrants: • Right Upper Quadrant • Right Lower Quadrant • Left Upper Quadrant • Left Lower Quadrant • Three central areas: • Epigastric • Periumbilical • Suprapubic
Location • RUQ pain - • duodenal ulcers, acute pancreatitis, acute cholecystitis, and acute hepatitis • LUQ pain - • gastritis, gastric ulcer, acute pancreatitis, and splenic infarct or rupture • RLQ pain - • acute appendicitis, • LLQ pain - • diverticulitis • GYN and urologic causes of acute abdominal pain can also present with lower quadrant abdominal pain
Radiation of Abdominal Pain • Perforated Ulcer • Biliary Colic • Renal Colic • Dysmenorrhea/Labor • Renal Colic (Groin)
Character • Implies all the features of the pain • Usually can be determined by asking the patient to describe the quality of the pain • Most often described as • sharp or dull • cramping (colicky)
Character • Colicky pain - rhythmic pain resulting from intermittent spasms - most commonly associated with • biliary disease, nephrolithiasis, intestinal obstruction • Pain that begins as dull, poorly localized ache and progresses to a constant, well localized sharp pain indicates a surgically correctable cause
Physical Examination of the Abdomen • Inspection • Auscultation • Percussion • Palpation
Inspection • General observation • Look at abdominal contour, note location of any scars, rashes or lesions
Inspection • Patient writhing in agony - likely has colicky abdominal pain caused by ureteral lithiasis • Patient lying very still - more likely to have peritonitis • Patient leaning forward to relieve pain - may have pancreatitis
Inspection • The abdominal wall is a commonly overlooked source of abdominal pain • Other parts of the body should also be inspected. For example, the eyes should be inspected for evidence of scleral icterus which may indicate hepatobiliary disease
Auscultation • Useful in assessing peristalsis • Bowel sounds are widely transmitted through the abdomen - therefore, it is not necessary to listen in all 4 quadrants • Auscultation should last at least 1 minute • Bowel sounds typically highly pitched so the diaphragm of the stethoscope should be used
Auscultation • ? Bowel sounds- normal/hyperactive/hypoactive • Auscultation should precede percussion and palpation • ? Abdominal bruits - • listen over aortic,iliac and renal arteries
Auscultation • Hypoactive bowel sounds - associated with ileus, intestinal obstruction, peritonitis • Intestinal obstruction can produce hyperactive bowel sounds which are high pitched tinkling sounds occurring at brief intervals; very audible
Percussion • Technique - performed by firmly pressing the index finger of one hand on the abdominal wall while striking the abdominal wall with the other index finger • Percussion note can be described as dull, resonant, or hyperresonant
Percussion • Dull/resonant or hyperresonant • Tympany normally present in supine position • ? Unusual dullness • ? Clue to underlying abdominal mass
Percussion • Gastric region - • percussion over the gastric region will generate a hyperresonant note because of usual presence of a gastric air bubble • Liver - • percussion over the liver will generate a dull note • A normal liver span is 6 to 12 cm in the midclavicular line
Percussion • Generalized percussion is a useful method for detecting the presence of ascites or intestinal obstruction in a distended abdomen • In ascites - a dull percussion note would be generalized • In intestinal obstruction - a hyperresonant note would be heard
Percussion • If ascites is suspected, then a test for shifting dullness can be performed • Ascites typically sinks with gravity, percussion of the flanks generates a dull note and percussion of the periumbilical region generates a resonant note in the supine patient
Percussion • The test for shifting dullness involves having the patient shift to a lateral decubitus position and then performing percussion again; the area of resonance should shift upward
Shifting Dullness • If dullness on percussion shifts when the patient is rolled on the side, peritoneal fluid (ascites) may be present.
Percussion • Splenic Enlargement A change from tympany to dullness suggests splenic enlargement
Palpation • Before palpating the abdomen the examiner should ask the patient to point directly to the area that hurts most and avoid palpating that area until absolutely necessary • May be difficult in patient who has guarding (voluntary or involuntary)
Palpation • Voluntary guarding - conscious elimination of muscle spasms • Involuntary guarding - reported when the spasm response cannot be eliminated, which usually indicates diffuse peritonits
Palpation • Where is pain ? Begin with light palpation • Guarding - voluntary/involuntary • Rebound tenderness
Palpation • Rebound tenderness is elicited by pressing on the abdominal wall deeply with the fingers and then suddenly releasing the pressure • Pain on the abrupt release of steady pressure indicates the presence of peritonitis • Asking the patient to cough is another method of eliciting signs of peritonitis
Rebound Tenderness • This is a test for peritoneal irritation. Palpate deeply and then quickly release pressure. If it hurts more when you release, the patient has rebound tenderness
Deep Palpation • ? Areas of deep tenderness/masses
Palpation of Aorta • Easily palpable on most • Pulsate with deep palpation of central abdomen • Enlarge aorta - • ? Sign of aortic aneurysm
Palpation of Spleen • Not normally palpable
Costovertebral Angle Tenderness • CVA tenderness is often associated with renal disease. Use the heel of your closed fist to strike the patient firmly over the costovertebral angles
Specific Disorders • Upper abdominal pain - common causes of acute abdominal pain in the upper abdomen include: acute cholecystitis, acute pancreatitis, perforated ulcers • Pain usually overlaps the left and right upper quadrants
Classic Presentations - Acute Cholecystitis • Localized or diffuse RUQ pain • Radiation to right scapula • Vomiting and constipation • Low grade fever
Cholecystitis • Murphy’s sign (have patient take a deep breath while right subcostal area is palpated) abrupt cessation of inspiration secondary to pain is considered a positive Murphy’s sign • Disease of adulthood • More common in women • Bacteria invasion can develop into ascending cholangitis • Charcot’s triad • Right upper quadrant pain • Fever • Jaundice
Acute pancreatitis • Retroperitoneal dissection of blood can result in bluish discoloration of the flanks (Turner’s sign) or of the periumbilical region (Cullen’s sign) • Biliary pancreatitis secondary to cholelithiasis is most common women > age 50 in community hospital setting • Alcoholic pancreatitis is most common in men ages 30-45 years in urban hospital setting • Symptoms-epigastric pain,nausea,vomiting,pain is constant & boring in nature • Bowel sounds decrease - lack of rigidity or rebound tenderness
Perforated Peptic Ulcer • Sudden onset - severe epigastric pain • Pain becomes generalized after a few hours to involve the entire abdomen • Perioperative mortality rate of 23% • Patient usually lying quietly and breathing shallow. • Abdomen rigid,board-like, guarding - maximal at site of perforation • Upright chest x-ray - detection of free intraperitoneal air
Specific Disorders • Midabdominal pain - common causes of midabdominal pain include • intestinal obstruction, mesenteric ischemia and early appendicitis • dissecting aortic aneurysm • myocardial infarction
Intestinal Obstruction • Mechanical - results from • gallstones, adhesions, hernias, volvulus, intussuseption, tumors • Non-mechanical- results from • intestinal infarction or occurs after surgery as a paralytic ileus, pain medication