Download
1 / 125
1.34k likes | 1.78k Views
Pathophysiology of Urinary Tract Obstruction chapter 40. Dr.Mariam Malallah Dr.Abdullatif Al-Terki. Obstruction of the urinary tract. Obstruction of the urinary tract can occur during fetal development, childhood, or adulthood.

E N D
Pathophysiology of Urinary Tract Obstructionchapter 40 Dr.Mariam MalallahDr.Abdullatif Al-Terki
Obstruction of the urinary tract • Obstruction of the urinary tract can occur during fetal development, childhood, or adulthood. • The point of obstruction:Proximal -> calyces Distal -> urethral meatus. • lead to permanent renal damage limiting the excretion of metabolic wastes altering water and electrolyte balance.
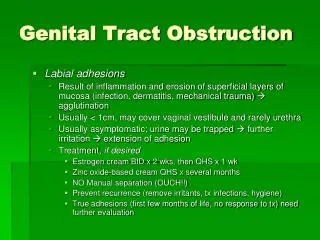
Hydronephrosis:- Is the dilation of the renal pelvis or calyces. - Associated with obstruction. - may be present in the absence of obstruction. • Obstructive uropathy:- The functional or anatomic obstruction of urinary flow at any level of the urinary tract. - The obstruction causes:functional or anatomic renal damage.
GLOBAL RENAL FUNCTIONAL CHANGESGlomerular Filtration, Renal Blood Flow, Collecting System Pressure • Functional changes associated with obstructive nephropathy. - Renal hemodynamic variables- Glomerular filtration. • influenced by:- The extent and severity of obstruction- Unilateral or bilateral- Persists or has been relieved.
Factors influencing GFR are expressed in the following equation: GFR = Kf (PGC −PT −πGC) • Kf: glomerular ultrafiltration coefficient • PGC: glomerular capillary pressureInfluenced by:- Renal plasma flow (RPF)- The resistances of the afferent and efferent arterioles. • The hydraulic pressure of fluid in the tubule (PT) • oncotic pressure (π) of the proteins
RPF depends upon: - The renal perfusion pressure - Intrarenal resistance to flow is mediated by the resistances in the afferent and efferent arterioles. RPF = aortic pressure − renal venous pressure renal vascular resistance • Obstruction can transiently or permanently alter GFR and some or all of the determinants of GFR.
Unilateral and bilateral ureteral obstructions differ in- the patterns of hemodynamic- ureteral pressure changes- distribution of renal blood flow.
Hemodynamic Changes with Unilateral Ureteral Occlusion • Animal experiments have demonstrated a triphasic pattern of RBF and ureteral pressure changes in UUO • first 1 to 2 hours-RBF increases -high PT and collecting system pressure • second phase lasting 3 to 4 hours-pressure parameters remain elevated-RBF begins to decline. • third phase beginning about 5 hours after obstruction -a further decline in RBF-decrease in PT and collecting system pressure.
Triphasic relationship between ipsilateral renal blood flow and left ureteral pressure during 18 hours of left-sided occlusion. • The three phases are designated by roman numerals and separated by vertical dashed lines. • In phase I, renal blood flow and ureteral pressure rise together. • In phase II, the left renal blood flow begins to decline and ureteral pressure remains elevated and, in fact, continues to rise. • In phase III, the left renal blood flow and ureteral pressure decline together.
It is likely that both PGE2 and NO contribute to the net renal vasodilation that occurs early following UUO. • Thus reduced whole kidney GFR at this stage of obstruction is due not only to reduced perfusion of individual glomeruli, related to afferent vasoconstriction and reduced PGC,but also to global reduction in filtration related to no perfusion or underperfusion of many glomeruli.
Hemodynamic Changes with Bilateral Ureteral Occlusion • A modest increase in RBF with BUO that lasts approximately 90 minutesfollowed by a prolonged and profound decrease in RBF that is greater than found with UUO. • The intrarenal distribution of blood flow is quite different with BUO than with models of UUO. • Thus the shift seen with UUO of blood flow from outer to inner cortex is the opposite of that with BUO.
Ureteral pressure is higher with BUO than with UUO. • Inboth cases ureteral and tubular pressures are increased for the first 4 to 5 hours.-The ureteral pressure remains elevated for at least 24 hours with BUO-The ureteral pressure begins to decline and approaches preocclusion pressures by 24 hours with UUO.
This difference between the two pathophysiologic conditions has been hypothesized to be -due to an accumulation of vasoactive substances in BUO that could contribute to preglomerular vasodilation and postglomerular vasoconstriction. -Such substances would not accumulate in UUO because they would be excreted by the contralateral kidney. E.g. Atrial natriuretic peptide (ANP)
In summary, • both UUO and BUO involve increases in renal vascular resistances and increases in ureteral pressures. the timing and regulation of these changes differ • With UUO, early renal vasodilation primarily mediated by prostaglandins and NO is followed by prolonged vasoconstriction and normalization of intratubular-ureteral pressure as the contralateral kidney contributes to fluid balance. • With BUO, little early vasodilation is seen, and vasoconstriction is more profound. When the obstruction is released, the postobstructive diuresis is much greater with BUO because volume expansion, urea and other osmolytes, and secreted ANP contribute to a profound diuresis and natriuresis.
Partial Ureteral Occlusion • Formation of glomeruli and tubules may be compromised so that irreversible changes occur without total loss of kidney function. • Partial neonatal obstruction can impair nephrogenesisindependently of renal functional decline • these changes may depend upon : -species-stage of renal development-degree of occlusion.
Egress of Urine from the Kidney • urine may still egress from the kidney. • extravasation at the calyceal fornix (pyelosinus) that occurs with acute obstruction, typically ureteral stones. • Extravasation of urine into the venous (pyelovenous) and lymphatic system (pyelolymphatic) • In chronic obstruction, fluid is thought to exit into the renal venous system.
Effects of Obstruction on Tubular Function • Postobstructive diuresis:- Commonly after reversal of BUO - uncommonly after release of UUO probably as a consequence of the contralateral renal unit’s functional capacities that are enhanced by an upregulation of ion transporters
Urinary Concentrating Ability • Normal urine concentrating ability requires:- Hypertonic medullary interstitial gradient because of active salt reabsorption from the thick ascending limb of Henle. - Urea back flux from the inner medullary collecting duct - Water permeability of the collecting duct mediated by vasopressin and aquaporin water channels. • Obstructive nephropathy can disrupt some or all of these mechanisms.
Thus dysregulation of aquaporin water channels contribute to the long-term polyuria and impaired concentrating capacity • These defects are enduring and correct slowly with time.
Sodium Transport • Although ANP appears to play a role in sodium diuresis after release of BUO, it is unlikely to affect sodium transport defects associated with UUO. • Sodium excretion is greater after relief of BUO because extracellular volume is expanded and ANP directly affects transport and glomerular filtration.
The sodium transport defects associated with UUO is most likely due to selective cell membrane changes in the nephron that reduce the number and effectiveness of sodium transporters. Such changes may also occur with BUO. • Ischemia can also be a mediator of reduced transporter expression. • changes in renal interstitial pressure and local generation of natriuretic substances. • Thus substrate delivery may be a regulatory step in the expression of sodium and possibly other transporters. • Intrarenal and extrarenal substances and hormones can also modulate sodium transport. E.g. PGE2 in the renal medulla • The FENa following relief of BUO is typically greater than that after UUO because BUO causes retention of Na, water, urea nitrogen, and other osmolar substances and increased production of ANP, all of which stimulate a profound natriuresis.
Potassium Transport • Potassium and phosphate excretions follow changes in sodium; they are decreased with UUO because of altered transporters and postobstructive retention and increased transiently with BUO in parallel with the massive natriuresis. • there is a decrease in K+ excretion, with the relief of UUO.-due to reduced delivery of Na+ to the distal nephron -low volume flow rate that would minimize the transmembrane gradient for K+ secretion. -an intrinsic defect in K+ secretion • K+ excretion increases , with the relief of BUO. -due to the massive increases in Na+ and water delivery to the collecting duct acting as stimuli to secretion- also to the presence of high levels of ANP that can stimulate K+ secretion in the distal nephron
Hydrogen Ion Transport and Urinary Acidification • Obstruction causes a deficit in urinary acidification that has been demonstrated in human subjects as well as animal models. • A number of causes for the lack of acidification, including:- defects in H+-ATPase or H+- K+-ATPase- Cl−/HCO3− exchange- Back leak of protons into the renal interstitium- Failure to generate a satisfactory transluminal electrical gradient.
Effects of Obstruction on Anion and Other Cation Transport • The effects on phosphate reabsorption after the release of obstruction vary depending upon whether it was bilateral or unilateral. • When BUO is released, accumulated phosphate is rapidly excreted in proportion to sodium • Conversely, a decrease in phosphate excretion and a net retention occur with release of UUO. • Magnesium excretion is markedly increased after the release of either UUO or BUO. • calcium excretion may be increased or decreased, depending to a degree on the type of obstruction and the species.
Effect of Obstruction on the Excretion of Peptides and Proteins • Changes in peptide excretion reflect mediators and markers of renal damage. • Monocyte chemoattractant protein 1- Its excretion in the urine after UUO increases - an index of tubular damage. • - Epidermal growth factor (EGF) excretion- The renal cortical and outer medullary concentration of pre-pro-EGF- The excretion of Tamm-Horsfall protein All decrease with obstruction. • Urinary enzymes derived from the proximal tubule, e.g. alkaline phosphatase, γ-glutamyltransferase, N-acetyl-β-D-glucosaminidase, and leucine aminopeptidase - elevated in patients with obstructed kidneys
Metabolic Determinants of Ion Transport • Renal obstruction provokes a number of changes in the metabolic cascade. • There is a shift from oxidative metabolism to anaerobic respiration. • This shift results in a reduction of renal ATP levels, an increase in amounts of adenosine diphosphate (ADP) and adenosine mono- phosphate (AMP), and an increase in the renal lactate- to-pyruvate ratio
Cellular and Molecular Mechanisms Leading to Tubular Cell Death through Apoptosis • Renal obstruction tubular atrophy and cell death. • Apoptosis triggered by both intrinsic and extrinsic factors degradation and condensation of the nucleus cells further degrades into apoptotic bodies phagocytized by healthy cells • Glomerular cells appear to be resistant to obstruction-induced apoptosis.
Caspases mediate apoptotic cell death in obstructed kidneys • Two distinct pathways of caspase 1- activation of membrane death receptors by extrinsic binding of tumor necrosis factor alpha (TNF-α) to its receptor. 2- involves intrinsic stress signals that result in mitochondrial release of proapoptotic proteins such as cytochrome c. • The two pathways activate effector caspases cleave nuclear and cytoplasmic components condensation of nuclear material cell death.
Angiotensin blockade or ACE inhibition has been shown by some investigators to reduce apoptosis in the early phases of renal obstruction • TNF-α can be a directly cytotoxic cytokine that can induce apoptosis in addition to its role in renal inflammation.
Cellular and Molecular Changes Leading to Fibrosis • Urinary tract obstruction leads to progressive and, eventually, permanent changes in the structure of the kidney, including:-tubulointerstitial fibrosis-tubular atrophy and apoptosis-interstitial inflammation. • In other words:Ureteral obstruction leads to renal inflammation, increased extracellular matrix formation, tubulointerstitial fibrosis, and apoptosis of renal tubule cells.
Although the events leading to fibrosis are thought to be initiated by increased angiotensin II, other profibrotic factors appear to play a significant role because inhibition of angiotensin synthesis by ACE inhibitors or antagonism of the AT1 receptors blunts but does not completely abolish the fibrotic process
Experimental Treatment Approaches to Attenuate Renal Fibrosis and Functional Impairment • These studies suggest an important role of angiotensin-mediated profibrotic and apoptotic events occurring with renal obstruction that can be reduced with currently available inhibitors of angiotensin synthesis or receptor blockade.
Compensatory Renal Growth • An increase in contralateral renal volume has been detected ultrasonographically when contralateral hydronephrosis or unilateral renal agenesis is present. • influenced by several factors including:-age-degree of obstruction-duration of obstruction. • Both hyperplastic and hypertrophic CRG • Studies of humans subjected to nephrectomy, a functional surrogate for obstruction, have demonstrated that a reduction in CRG occurs with increasing age • less prominent with partial than with total UUO • While the kidney enlarges -an increase in the number of nephrons or glomeruli does not occur.
Insulin-like growth factor I (IGF- I) may play a role. • Other growth factors, cytokines, and enzymes may be involved in regulating CRG, including IGF binding protein–3 (IGFBP-3), vascular endothelial growth factor (VEGF), matrix metalloproteinase–9 (MMP-9), interleukin-10 (IL-10), and TGF-β • CRG may be influenced by mitochondrial respiration
Renal Recovery after Obstruction • When acute, complete ureteral obstruction is promptly relieved, full recovery of global GFR can occur. • Longer periods of complete ureteral obstruction are associated with diminished return of GFR.
Histopathological findings may predict recovery of renal function. • Renal parenchymal thickness based on computed tomography (CT) Further studies are needed to corroborate these results before this approach is used in clinical practice. • Other factors influence functional return Factors that have a positive influence on functional recovery include:- a smaller degree of obstruction- greater compliance of the collecting system- presence of pyelolymphatic backflow Predictors of diminished recovery of renal function -older age-decreased renal cortical thickness
Nuclear renography - is the best predictor. • For example:dimercaptosuccinic acid (DMSA), a cortical agent, has been shown to be superior to tubular selective agents, such as diethylenetriaminepentaacetic acid (DTPA) or mercaptoacetyltriglycine (MAG3), for the prediction of renal recovery
PATHOLOGIC CHANGES OF OBSTRUCTION • These may be affected by: -the presence of infection -duration of obstruction -intra versus extrarenal localization of the renal pelvis.
Gross Pathologic Findings • at 42 hours after obstruction :Dilation of the pelvis and ureter blunting of the papillary tips the weight of this renal unit heavier. • at 7 days. Pelviureteric dilationweight further increased parenchyma became edematous • at 12 daysThe cortex remained slightly enlarged increased calyceal dilatation • at 21 and 28 daysthe external renal dimensions of both kidneys were similar. the cortex and medullary tissue diffusely thinned. • At 6 weeksThe totally obstructed kidneys enlarged, had a cystic appearance, and weighed less than the contralateral renal unit The partially obstructed kidneys no gross differences in appearance
Microscopic Pathologic Findings • Widespread glomerular collapse and tubular atrophy, interstitial fibrosis, and proliferation of connective tissue in the collecting system were reported at 5 to 6 weeks after obstruction • This is believed to be a result of interplay of several cellular and molecular mechanisms that collectively lead to the subtle development of tubular atrophy, macrophage infiltration/proliferation in the renal interstitial tissue, interstitial fibrosis and progressive loss of nephrons
Electron Microscopic Pathologic Findings • Including:-tubular atrophy-glomerular collapse-renal pelvic smooth muscle atrophy at 5 to 6 weeks after obstruction • other changes including:-a cell-poor stroma composed of elastic and collagen fibers in the renal interstitium-obstructed portions of the collecting system.
GENERAL ISSUES IN MANAGEMENT OF PATIENTS • Diagnostic Imaging • Ultrasonography • excretory urography (EXU) • retrograde pyelography • antegrade pyelography • isotopic renograph • computed tomography (helical) • magnetic resonance imaging • pressure flow study (Whitaker test).
Ultrasonography • Although it is primarily an anatomic study, Doppler modifications may add a functional component. • A prospective study of ultrasonography in obstruction revealed a 35% false-negative rate in acute obstruction, underscoring the need to correlate the clinical picture carefully with the radiologic findings.
Doppler ultrasonography allows measurement of the renal resistive index (RI), which has been used to assess for obstruction. The RI is defined as peak systolic velocity (PSV) minus the end-diastolic velocity (EDV) divided by the PSV. • values greater than 0.7 reflecting elevated resistance to blood flow and thus suggesting obstructive uropathy. • Although the presence of hydronephrosis associated with an abnormally elevated RI may be indicative of the severity of obstruction
Excretory Urography • the “gold standard” for the evaluation of the upper urinary tract • Advantages: it provides both anatomic and functional information: • Disadvantages: • the utility of EXU is limited in those with renal insufficiency. • risk of contrast nephropathy increases with increasing serum creatinine. - Radiation exposure limits its utility in pregnancy