Download
1 / 24
270 likes | 597 Views
Acoustic Neuroma Department of Otorhinolaryngoglogy the 2nd Hospital affliatted to Medical college Zhejiang University Xu Yaping. Anatomy Cerebellopontine Angle -CPA (in the posterior fossa). Epidemiology. 6 % of all Intracranial tumors 80 - 90% of CPA tumors

E N D
Acoustic Neuroma Department of Otorhinolaryngoglogy the 2nd Hospital affliatted to Medical college Zhejiang University Xu Yaping
Epidemiology • 6 % of all Intracranial tumors • 80 - 90% of CPA tumors • Incidence in US: 10 per million / year • Vast majority in adulthood • 95% Sporadic (unilateral) • 5% Neurofibromatosis type 2 (bilateral) • No known race, gender predilection
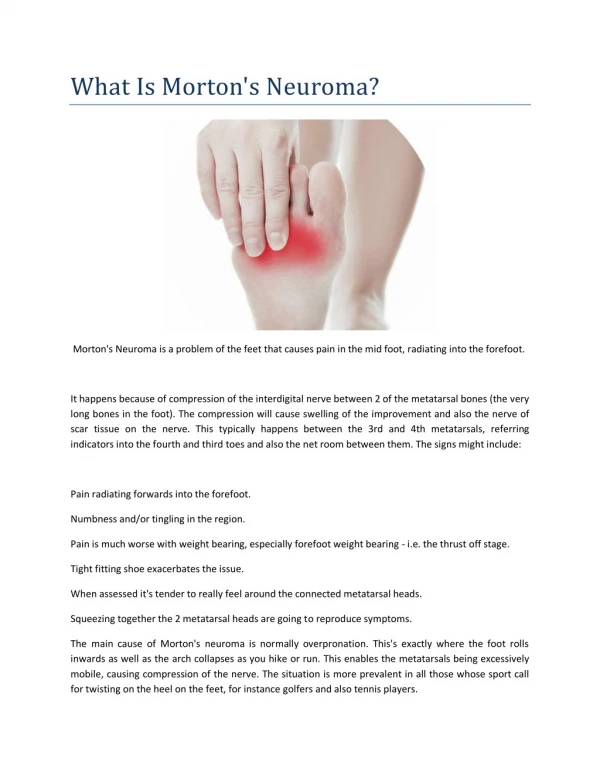
Pathogenesis • Neither neuroma or acoustic (auditory) • Schwannoma arising from vestibular nerve • Benign tumor. Malignant degeneration exceedingly rare. • Majority originate within the IAC(the internal auditory canal) • Equal frequency on Superior and Inferior vestibular nerves (controversial)
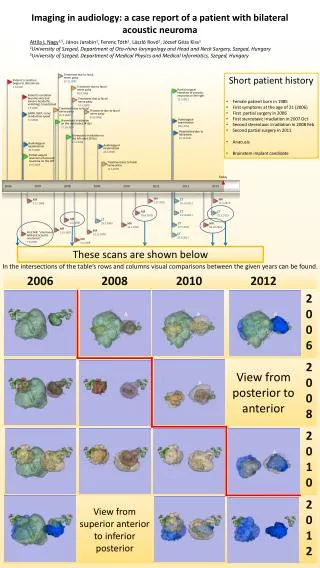
Phases of Tumor Growth • Intracanalicular: • Hearing loss, tinnitus, vertigo • Cisternal: • Worsened hearing and dysequilibrium • Compressive: • Occasional occipital headache • CN V: Midface, corneal hypesthesia • Hydrocephalic: • Fourth ventricle compressed and obstructed • Headache, visual changes, altered mental status
Intracanalicular Cisternal Hydrocephalic Compressive
Hearing Loss • Most frequent initial symptom • Most common symptom ~ 95% AN patients • Asymmetric SNHL • Down-sloping / High Frequency • Decreased Speech Discrimination • Lack of conclusive correlation between tumor size and hearing
Estimating Tumor Growth • Serial MRI with and without GAD(Gadolinium) ---The only reliable study to estimate tumor growth rate • Gadolinium-enhanced MRI remains the gold standard ---It can detect tumors as small as 1 mm and differentiate AN from many CPA lesions
Delayed Diagnosis Duration of Symptoms Prior to Diagnosis Symptoms Years • Hearing Loss 3.9 • Vertigo 3.6 • Tinnitus 3.4 • Headache 2.2 • Dysequilibrium 1.7 • Trigeminal 0.9 • Facial 0.6 ----Jackler RK. 2000. Tumors of the Ear and Temporal Bone
History and Physical • Hearing Loss • Vertigo • Dysequilibrium • Tinnitus • Headache • Nystagmus • Early small lesion: Horizontal (vestibular) • Late large: Vertical (brainstem compression) • Cranial neuropathy • CN V, VII • Lower cranial nerves (IX-XII)
Sudden Sensorineural Hearing loss • Idiopathic • 1-2 % SSNHL patients have AN • 10- 26 % AN patients have a history of SSNHL • Most experts advocate obtaining MRI in all patients who present with SSNHL
Diagnosis • History and Physical Exam • Audiology testing: • Audiogram • ABR • OAE • Vestibular testings (eg. ENG, rotary chair, posturography) all lack diagnostic value • Radiography • MRI Gold Standard • CT
ABR: Retrocochlear Pathology(Auditory Brainstem Response) • Increased interpeak intervals • I-to-III interval of 2.5 ms, III-to-V interval of 2.3 ms, and I-to-V interval of 4.4 ms • Interaural wave V latency difference (IT5) • Greater than 0.2 ms • Poor waveform morphology ie. only some of the waves are discernible • Absent waveform
ABR patterns in AN • 10-20 % with only wave I • and nothing thereafter • 40-60 % with wave V • latency delay • 10-15 % have normal • findings
OAE(Otoacoustic emissions) • Reflect cochlear/ OHC / sensory hearing • Not primarily used as screening tool • Presence of OAE in SNHL ↔ Retrocochlear • However, 50 % AN demonstrate both cochlear and retrocochlear hearing loss • Risk stratification for hearing preservation surgery
MRI Brain w. & w/o GAD T1 pre-Gad T2 T1 post-Gad T1: Isointense to brain, hyperintense to CSF T2: Hyperintense to brain, hypointense to CSF T1+Gad: Enhancing
CT Brain with contrast • Heterogeneous • enhancement on contrast • 2. Rare calcification • 3. Contraindication to MRI (metallic implants), claustrophobic patients • 4. May not be able to detect small tumor < 1.5cm • 5. Radiation
Treatment options • Observation<5mm • Surgery : >1cm • Translabyrinthine • Retrosigmoid • Middle fossa • Radiotherapy • Conventional • Stereotactic: knife <1-2cm
Conservative Management • Advanced age (> 65 ) • Short life expectancy (< 10 years) • Slow growth rate • Poor surgical candidate / poor general health • Minimal symptoms • Only hearing ear • Patience preference
Conclusions • Tumor size has no correlation with audiovestibular symptoms in Acoustic neuroma • Understanding tumor growth rate is important for predicting symptom progression and treatment planning • The study-of-choice to estimate tumor growth is serial MRI