Download
1 / 20
200 likes | 323 Views
The Unexpected Weak Auto Control. Alexander Delk, MT(ASCP)SBB CM Reference Laboratory Specialist. June 6, 2013. Objectives. 1. Recognize that a weak auto control can have more than one cause 2 . Emphasize the benefit of autologous adsorption

E N D
The Unexpected Weak Auto Control Alexander Delk, MT(ASCP)SBBCM Reference Laboratory Specialist June 6, 2013
Objectives • 1. Recognize that a weak auto control can have more than one cause • 2. Emphasize the benefit of autologous adsorption • 3. Recognize some medical conditions that can effect antigen expression
Case Study 93 year old Caucasian male Diagnosis: Leukemia Hb: 7.0 g/dL History of Anti-k Last transfusion 6 months ago DAT: IgG +w, C3 neg Phenotype: D+C+E-c-e+; K+k-; Fy(a+b+); Jk(a+b+); M+N+S+s+ We start with a selected cell panel
Selected Cells 1 Unexpectedly, all cells reacted 2+-3+ with a +w auto control.
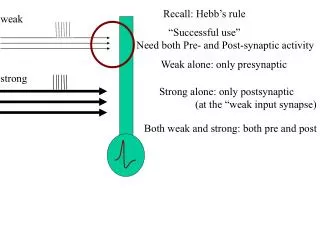
DAT Test to detect in vivo coating of red cells with immunoglobulin and/or complement. Small amounts of IgG and complement appear to be present on all red cells, but at levels undetectable with routine testing.
Some Causes of a Positive DAT Autoantibodies Serologic Transfusion Reactions Drug-induced antibodies Passively acquired alloantibodies Nonspecifically adsorbed proteins Complement activation due to bacterial infection, autoantibodies, alloantibodies Antibodies produced by passenger lymphocytes(transplants)
Discussion Double check the transfusion history Suspect additional alloantibodies, a high or multiple uncommon Treat the phenotype similar cells with ficin or 0.2M DTT Since the DAT and Auto Control are substantially weaker than the other cells tested, autoantibodies, while possible, seem unlikely.
Phenotype similar cells treated panel Well, no negatives, but we know that the target antigen is not destroyed by ficin or 0.2M DTT.
Discussion of the results Since both ficin and 0.2M DTT treated cells react, most likely not: MNS; Kell(system); LW; Ge2, Ge4; Lutheran; Dombrock; Yt These are still suspect: Rh; Diego; Co; Ge3; P; Jra; Lan; Vel
Type the patient for Highs The patient types R1R1,Co(a+), Di(b+), Ge: 2, PP1pk+, Jr(a+), Lan+, and Vel+ Although a few suspects remain, we start to consider autoantibodies. A LISS panel is tested to see if the reactivity diminishes. An eluate is prepared and tested with reagent cells and chloroquine treated DAT negative patient cells.
LISS Panel/Eluate Maybe it is a Warm Auto let’s try adsorptions!
Selected Cells with (homologous ZZAP) adsorbed Plasma There is an underlying Anti-E
Discussion of the results We did not have enough autologous cells for adsorption, so we performed phenotype matched (by ZZAP) homologous adsorptions. The weak DAT still concerned us. Since the patient is stable, we request additional samples to perform an autologous adsorption the following day.
Discussion Most agree that autoadsorption is the preferred technique. In this case(weak DAT), the autoadsorption if successful will allow us to be more confident in our identification. Autoadsorption may prove valuable even if the patient has been recently transfused. We can use such adsorbed plasma to rule in antibodies, but we must rely on other adsorption methods for rule outs.
Selected Cells with (autologous) adsorbed Plasma. Identical results! There is an underlying Anti-E
Interpretation This patient’s sample contains warm autoantibodies with diminished target antigen present on his RBCs. The patient has a history of Anti-k. Anti-E was also identified in the current sample.
Discussion The following are some medical conditions associated with diminished or altered antigen expression: Pregnancy, Carcinoma, Leukemia, Infections, Hodgkin’s disease, Thalassemia, PNH, AIHA, SLE, AIDS, Old age
Discussion In some cases there may be a complete suppression of the target antigen with a negative DAT and auto control. Kell (esp. Kpb), Rh, (D,e,hrS,hrB,Hr,Hro), and others have been implicated or suspected in transfusion reactions and/or clearance of the transfused RBCs. When we suspect this, we antigen type the patient for the particular antigen or several antigens within a system.
Conclusion Two units of E-,k- blood were transfused to the patient without incident. Questions?
References Daniels GL. Human blood groups. Oxford, UK: Blackwell Science, 2002. Issitt PD, AnsteeDJ. Applied Blood Group Serology 4th ed. Montgomery Scientific Publications. Reid ME, Lomas-Francis C. Blood group antigen facts book.2nd ed. San Diego: Academic Press, 2004.