Download
1 / 1

E N D
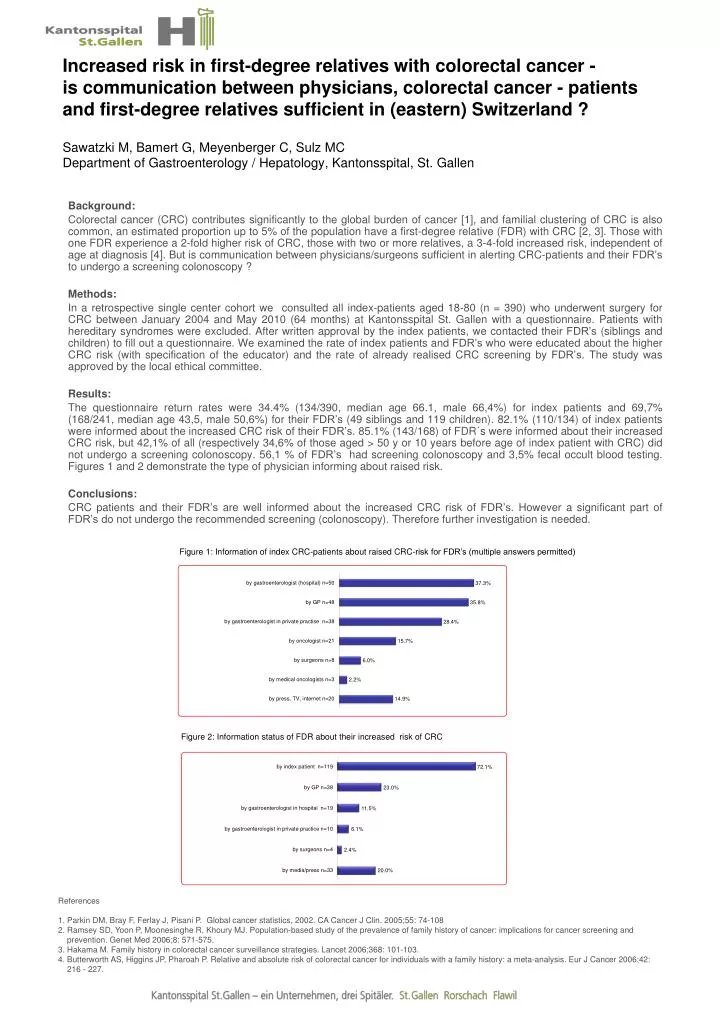
Increased risk in first-degree relatives with colorectal cancer - is communication between physicians, colorectal cancer - patients and first-degree relatives sufficient in (eastern) Switzerland ? Sawatzki M, Bamert G, Meyenberger C, Sulz MCDepartment of Gastroenterology / Hepatology, Kantonsspital, St. Gallen Background: Colorectal cancer (CRC) contributes significantly to the global burden of cancer [1], and familial clustering of CRC is also common, an estimated proportion up to 5% of the population have a first-degree relative (FDR) with CRC [2, 3]. Those with one FDR experience a 2-fold higher risk of CRC, those with two or more relatives, a 3-4-fold increased risk, independent of age at diagnosis [4]. But is communication between physicians/surgeons sufficient in alerting CRC-patients and their FDR’s to undergo a screening colonoscopy ? Methods: In a retrospective single center cohort we consulted all index-patients aged 18-80 (n = 390) who underwent surgery for CRC between January 2004 and May 2010 (64 months) at Kantonsspital St. Gallen with a questionnaire. Patients with hereditary syndromes were excluded. After written approval by the index patients, we contacted their FDR’s (siblings and children) to fill out a questionnaire. We examined the rate of index patients and FDR’s who were educated about the higher CRC risk (with specification of the educator) and the rate of already realised CRC screening by FDR’s. The study was approved by the local ethical committee. Results: The questionnaire return rates were 34.4% (134/390, median age 66.1, male 66,4%) for index patients and 69,7% (168/241, median age 43,5, male 50,6%) for their FDR’s (49 siblings and 119 children). 82.1% (110/134) of index patients were informed about the increased CRC risk of their FDR’s. 85.1% (143/168) of FDR´s were informed about their increased CRC risk, but 42,1% of all (respectively 34,6% of those aged > 50 y or 10 years before age of index patient with CRC) did not undergo a screening colonoscopy. 56,1 % of FDR’s had screening colonoscopy and 3,5% fecal occult blood testing. Figures 1 and 2 demonstrate the type of physician informing about raised risk. Conclusions: CRC patients and their FDR’s are well informed about the increased CRC risk of FDR’s. However a significant part of FDR’s do not undergo the recommended screening (colonoscopy). Therefore further investigation is needed. Figure 1: Information of index CRC-patients about raised CRC-risk for FDR’s (multiple answers permitted) Figure 2: Information status of FDR about their increased risk of CRC • References • 1. Parkin DM, Bray F, Ferlay J, PisaniP. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55: 74-108 • 2. Ramsey SD, Yoon P, Moonesinghe R, Khoury MJ. Population-based study of the prevalence of family history of cancer: implications for cancer screening and • prevention. Genet Med 2006;8: 571-575. • 3. Hakama M. Family history in colorectal cancer surveillance strategies. Lancet 2006;368: 101-103. • 4. Butterworth AS, Higgins JP, Pharoah P. Relative and absolute risk of colorectal cancer for individuals with a family history: a meta-analysis. Eur J Cancer 2006;42: • 216 - 227.