Download
1 / 53
600 likes | 2.08k Views
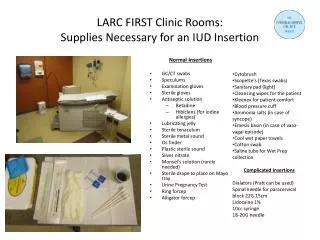
Betadine. Providone Iodine Used to “dry out” dry gangrene Goal is to keep dry gangrene contained and free of outside bacteria Cytotoxic. Dakin’s Solution. Diluted bleach Completely cytotoxic No known resistance, but no healing occurs Never use >48-72 hours. Acetic Acid. Diluted vinegar

E N D
Betadine • Providone Iodine • Used to “dry out” dry gangrene • Goal is to keep dry gangrene contained and free of outside bacteria • Cytotoxic
Dakin’s Solution • Diluted bleach • Completely cytotoxic • No known resistance, but no healing occurs • Never use >48-72 hours
Acetic Acid • Diluted vinegar • Excellent for pseudomonas aeruginonoa • Used during pulse lavage followed by NS rinse • Lymphedema patients=because of the rich protein, pts are prone to getting cellulitis.
Polyhexamethylene biguanide (PHMB) • Lavasept, Serasept (used to prep skin for s(x) • Broad spectrum • Used in foam dressing • Kill bacteria in drainage • More preventative measure than treatment • Kendall AMD, Suprasorb X + PHMB
Cadexomer Iodine • Providone Iodine combined with cadexomer starch • Allows for a slow, sustained release • Cytotoxic to bacteria, but low levels not cytotoxic to healing cells • Iodosorb
Topical Ointments • Silver sulfadiazine (Silvadene, burn cream) • Collagenase (Santyl) • Metronidazol Gel (MetroGel) • Mupirocin (Bactroban) • Bacitracin, neomycin, polymixin B (Triple antibiotic ointment, Neosporin)
Silver Sulfadiazine • Silvadene, burn cream • Sulfonamide plus antimicrobial silver • Cant tolerate the concentration needed to kill some bacteria. • It’s all we had for a long time • It is cytotoxic • Particularly beneficial for: • Pseudomonas • Acute burns
Silver Sulfadiazine • It’s cytotoxic – particularly to fibroblasts • Do not use >2 weeks • 2008 Cochrane Review • Prolongs healings • Not recommended for use • Allergic reactions to sulfa • Burning and pain when applied
Collagenase • Enzymatic debridement (Santyl) • Digests necrotic collagen • Specific and selective for denatured collagen • Effective when used for long periods of time • Maintenance debridement=when gets down to healthy, helps prevent slough from building up.
Collagenase • Considerations • Cost • Slow acting • Deactivated when combined with heavy metals • Silver
Metronidazole gel • MetroGel • Beneficial for anaerobic contamination • Fungatingwounds (end stage breast cancer, tumor is evasive and grows out, highly vascularized. • Can be combined with Mupirocin to treat MRSA • Helps with order control from wound.
Mupirocin • Bactroban • Bacteriostatic (bacteria lives, but can’t replicate) or Bactericidal (kills the bacteria) • Gram positive organisms including MRSA • Resistance is developing
Bacitracin, Neomycin, Polymixin B • Triple antibiotic ointment, Neosporin • Available in ointment or powder • Powder can be combined with collagenase • Allergies becoming more common
How to Dress a Wound • Moist wound healing is best • Goal of a dressing is to maintain appropriate moisture level • If necessary, lightly fill a cavity • No “packing” • Creates too much pressure • Whatever goes in, how are you going to get it out?
How to Dress a Wound • Considerations • Cost/insurance • Ease of Pt or caregiver to perform • Can you see what your applying a dressing to? • Allergies
Gauze - Use • Any wound!
Gauze - Advantages • Many forms • 4x4, 2x2, strip gauze, roll • Versatile • Flat, opened, fluffed, filling/packing • Cheap • Readily available w/o Rx • Mechanical debridement • Can be used with any topical or solution
Gauze - Disadvantages • Traumatic/painful removal • Dries out easily • Does not keep outside bacteria out • May require a secondary dressing • Leaves debris in wound bed, particularly if cut • Frequent use, longer need affects cost
Foams - Use • Stage II-IV pressure ulcers • PT, FT wounds • Infected or non-infected • Donor sites • Minor burns • Moderate to heavily exudating (Ins requirement)
Foams - Advantages • Options • Bordered vs non-bordered • Adhesive vs non-adhesive • Silver impregnated • Sheets, ropes • Moderate to heavy drainage • Safe under compression wraps
Foams - Disadvantage • Can macerate skin if drainage extends to wound border • Cost • Decreasing insurance reimbursement
Alginate/Hydrofiber - Use • Calcium alginate or synthetic hydrofiber • Stage II-IV pressure ulcers • PT, FT wounds • Moderate to heavily exudating • Tracts, undermining • Infected wounds
Alginate/Hydrofiber - Advantages • Keeps wound bed moist • Can be impregnated with silver, Leptospermum honey • Hemostasis properties • Atraumatic removal when fully hydrated • Variety – sheets, ropes
Alginate/Hydrofiber - Disadvantages • Requires secondary dressing • Can dry out and adhere to wound • Can leave debris/lint • Can macerate unprotected skin
Collagen Donating - Use • Donate synthetic or porcine collagen to wound bed • Provides the scaffolding for cells to populate and migrate • Attracts cells to the wound site • Increase cellular proliferation • Any wound – but needs bountiful granulation tissue
Collagen Donating - Advantages • Non-adherent, comfortable • Can be left on up to 7 days, need to keep wet. • Can combine with lots of different products as long as still in contact with wound bed • Does lots of great stuff for the wound bed
Collagen Donating - Disadvantage • Cost $30-35 per sheet • Requires a clean, non-infected wound • Requires secondary dressing
Transparent Film - Use • Polyurethane with porous adhesive • Allows transmission of oxygen and moisture vapor • Can be primary or secondary dressing • Stage I or II pressure ulcers • Superficial burns • Donor sites
Transparent Film - Advantages • Visualize wound thru dressing • Impermeable to fluid and bacteria • Autolytic debridement (more on that later…) • Dressing can be on up to 7 days • Lots of different sizes • Silver impregnated available
Transparent Film - Disadvantage • Does not absorb drainage • Adheres to skin • Possible skin reaction • Can cause maceration
Hydrocolloid - Use • Primary or secondary dressing • Stage I, II pressure ulcers. Shallow stage III, IV • Not how deep, but rather how deep the bone is below. • PT, FT • Superficial burns • Hydrophilic colloid forms gel on contact with wound fluid • Impermeable
Hydrocolloid – Advantages • Maintain moist environment • Impermeable to moisture, bacteria • Autolytic debridement • Wear 3-7 days • Self adhering and conforms to any shape • Can be impregnated with silver
Hydrocolloid – Disadvantage • Minimal absorption • Contraindicated in presence of infection • Can be difficult to remove, skin tears • No undermining or tracking • Stinks! • Can NOT have any sign Infection.
Hydrogels - Use • Donate moisture to a wound • Non-crosslinked polymers plus water and/or glycerin • Can be impregnated with silver • Can be used in any type of wound • Many forms – gel, sheets • Gel can be used with any type of dressing
Hydrogels - Advantages • Great for donating moisture • Radiation burns: does permanent damage to skin for rest of life with be poor healing. • Autolytic debridement • Easily removed from wound without trauma • Can reduce pain
Hydrogels - Disadvantages • Potential for maceration • Requires daily changes • Requires secondary dressing • Unless bordered sheet • Sheets cannot be used with heavy drainage • Cannot act as a filler
Miscellaneous Dressings • Methylene blue and gentian violet • Absorptive, bacteriostatic • Hydrofera Blue • Leptospermum honey • Debridement, antimicrobial, many forms • Medihoney • Cutimed Sorbact • Hydrophilic dressing that traps bacteria, bacteriostatic
Modalities • 10-15% wound closure in one week is NORMAL wound healing • If failing to meet this on a regular basis…
Electrical Stimulation • One of the oldest >30 years • Strength of evidence: Level A • Medicare reimbursement only if wound is considered “chronic” • Traditional wound care >30 days without progress
Electrical Stimulation • How does it work in wounds? • Strong evidence it works, theory on how • “Current of Injury” • When cells are injured – they give off a negative charge • Believed that in chronic wounds – this is broken • Goal of e-stim is to mimic this current • Accelerate or “jump start” wound healing cascade
Electrical Stimulation • What does it do? • Stimulates fibroblasts, collagen synthesis • Increase receptor sites for growth factors • Improved tissue perfusion • Decreased edema • Increase tissue oxygen • Decrease pain • Increase tensile strength
Electrical Stimulation • High Volt Pulsed Current (HVPC) • Most commonly used for wound care • Monophasic waves • Studies show galvanotaxis occurs in wounds with cells required for tissue repair
Electrical Stimulation • Galvanotaxis by the Anode (+) • Neutrophil • Macrohages (acute inflammation) • Epidermal cells (end phase) • Endothelial cells
Electrical Stimulation • Galvanotaxis by Cathode (-) • Neutrophils (+ charged when wound is infected) • Fibroblasts • Need Fibroblasts for angiogenesis and proliferative phase of healing • ALWAYS START (-)!
Electrical Stimulation • Indications • Any type of wound • Contraindications • Basal or squamous cell carcinoma in area • Osteomyelitis • Suspected, new or if not responding to antibiotics • Pain, deep ache, infection of exposed bone, increased drainage, neuropathic and foot hurts. • Ion residue in wounds (e.g. silver) • Over electrical implants, over the heart or carotid artery, near laryngeal musculature
Electrical Stimulation • Duration: • 45-60 minutes • Frequency • 5-7 times/week done at home. • 100pps • Electrode placement • 12:00 and 6:00 • 3:00 and 9:00 • Dispersive pad about 30cm from wound • Saline moistened gauze in wound bed for conduction
Ultrasound • Contact ultrasound • Used in wound healing >50 years • Not so much recently • Non-contact ultrasound • Much more trendy • Next week
Ultrasound • High frequency • 3 MHz for superficial dermal wounds • 1 MHz for deeper structures and periwound 1 MHz = 3-5 cm depth 3 MHz = <2 cm
Ultrasound • Any stage of healing: • Pulsed mode • 20% duty cycle • Before application: • Cleanse periwound skin with mild soap and water and rinse well.