Download
1 / 33
340 likes | 506 Views
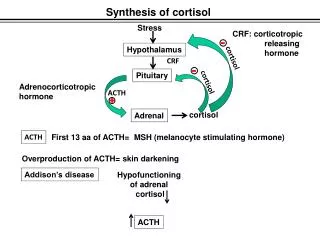
Measuring Urinary Free Cortisol. Release of Cortisol. Stress. -. Corticotrophin Releasing Hormone (CRH). The hypothalamus. -. Adrenocorticotropic Hormone (ACTH). Pituitary Gland. Cortisol. Adrenal Cortex. Suppress Immune Response. Increase Blood Glucose.

E N D
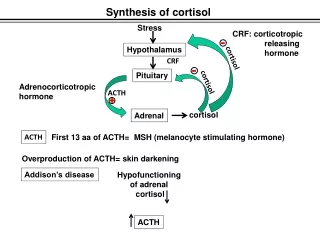
Release of Cortisol Stress - Corticotrophin Releasing Hormone (CRH) The hypothalamus - Adrenocorticotropic Hormone (ACTH) Pituitary Gland Cortisol Adrenal Cortex Suppress Immune Response Increase Blood Glucose Catabolism of proteins, fat.
Detection of Cushing’s Syndrome Cushing’s syndrome: A group of signs and symptoms caused by abnormally high levels of cortisol. Causes of Cushing’s syndrome: 1. Ingestion of exogenous steroids 2. A pituitary tumor that produces ACTH (also called Cushing’s disease) 3. Primary overproduction of cortisol by the adrenal gland due to an adrenal tumor or to adrenal hyperplasia. 4. Tumor outside of the hypothalamic-pituitary axis that produces ACTH (ectopic ACTH production)
Laboratory Tests Presentation of excess cortisol *24-hour urine test *Single low dose dexamethasone suppression test *Saliva or blood cortisol at 11 PM Differential Diagnosis of Cushing’s Syndrome (cause: pituitary, adrenal, or other) *High dose dexamethasone suppression test *ACTH levels *CRH stimulation test *Imaging tests
Presentation of excess cortisol . 24-hour Urine Cortisol (or urine free cortisol) sensitivity of 95-100%, specificity of 94-98%to detect cushing’s syndrome Since cortisol levels vary greatly over the course of a day, a single cortisol result is of little value and other ways of measuring overall cortisol production are used to evaluate overall cortisol production. . Saliva or blood cortisol at 11 PM . Single low dose dexamethasone suppression test The overnight low dose test consists of dexamethasone (1mg) taken orally between 2300 and 2400 hours, and the measurement of fasting plasma cortisol between 0800 and 0900 hours the following morning. Patients with all types of Cushing’s syndrome will not show adequate suppression after a single low dose of dexamethasone given at bedtime.
Differential Diagnosis of Cushing’s Syndrome (cause: pituitary, adrenal, or other) . ACTH levels . High dose dexamethasone suppression test Standard high dose DST: 2 mg 6-hourly for 8 doses. Plasma and/or urine cortisol are evaluated before, during and after dexamethasone administration High dose glucocorticoids partially suppress ACTH secretion from most corticotroph adenomas (80-90%) whereas ectopic tumours are resistant to feedback inhibition. . CRH Stimulation TestCRH (corticotrophin releasing hormone) is injected and cortisol and ACTH are measured at baseline (before CRH) and at 30 and 60 minutes. The normal response is a peak in ACTH levels at 30 minutes with cortisol peaking at 60 minutes. Most patients with Cushing’s syndrome caused by adrenal tumors or ectopic ACTH secreting tumors do not respond to CRH. . Imaging Tests CT (computed tomography) MRI (magnetic resonance imaging) Ultrasound
About 95% of cortisol is carried in the blood bound largely to Corticosteroid Binding Globulin (CBG) or albumin. The remainder occurs as physiologically active free cortisol. Around 1 percent of plasma free cortisol is secreted unaltered in the urine. Urinary free cortisol levels reflect the biologically active unbound hormone. Urinary free cortisol normal values are 20 to 100ug per 24 hours.
hydroxycortisol tetrahydrocortisol tetrahydrocortisone Urinary metabolites of cortisol
Routine methods for determination of urinary free cortisol Immunoassy: . less expensive and easily available . interfered with metabolites, precursor, other steroids with similar structures and steroid drugs . no internal standard to control extraction process HPLC: . more specific, separate interfering substances . internal standard to control extraction process . extensive sample preparation . long run time Develop LC-MS/MS methods
Sample preparation C18 SPE Column, 500mg Wash with 3ml of methanol 3ml of H2O Load samples Wash with 3ml of acetone:H2O (1:4) 3ml of H2O 3ml of hexane Elute with 3ml of diethyl ether Dry and reconstitute in mobile phase Journal of Chromatography, 426 (1988) 25-32.
LC MS/MS System Applied Biosystems/MDS Sciex API 3000™ LC/MS/MS System Triple quadrupole mass spectrometer
Triple Quadrupole mass spectrometry Series of three quadrupoles can be used, this is known as Triple Quadrupole mass spectrometry. The first and third quadrupoles are mass filters, and the middle one is a collision cell. This allows the study of fragments, useful in structural studies. For example, the first quadrupole may be set to "filter" for a drug ion of a known mass, which is fragmented in the second quadrupole. The third quadrupole can then be set to scan the entire m/z range, giving information on the sizes of the fragments made. Thus, the structure of the original ion can be deduced.
quadrupole The quadrupole consists of four parallel metal rods. Each opposing rod pair is connected together electrically and a radio frequency voltage is applied between one pair of rods, and the other. A direct current voltage is then superimposed on the R.F. voltage. Ions travel down the quadrupole in between the rods. Only ions of a certain m/z will reach the detector for a given ratio of voltages: other ions have unstable oscillations and will collide with the rods. This allows selection of a particular ion, or scanning by varying the voltages
(1) Product ion scan. In this case, the precursor ion is focussed in Q1 and transferred into Q2 - the collision cell - where it interacts with a collision gas and fragments. The fragments are then measured by scanning Q3. This results in the typical MS/MS spectrum and is the method most commonly employed with ESI ionisation and/or LC-MS.(2) Precursor ion scan. In this case Q3 is held to measure the occurrence of a particular fragment ion and Q1 is scanned. This results is a spectrum of precursor ions that result in that particular product ion - this is especially useful when used with EI or CI ionisation and/or GC-MS.(3) Neutral loss scan. In this case Q1 is scanned as in (2) but this time Q3 is also scanned to produce a spectrum of precursor ions that undergo a particular neutral loss. Again this mode is especially useful for EI and CI ionisation.
Standard cortisol + 11-deoxycortisol C18, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Urine blank C18, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Urine spiked with cortisol C18, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Urine spiked with 11-deoxycortisol C18, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Urine spiked with cortisol + 11-deoxycortisol C18, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Urine blank C18, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Urine blank C8, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Urine blank, left over weekends in r.t. C8, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Standard cortisol + 11-deoxycortisol C8, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Urine spiked with 11-deoxycortisol C8, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Urine spiked with cortisol C8, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
Urine spiked with cortisol+11-deoxycortisol C8, 98% methanol + 2% 5mM ammonium formate Cortisol 363.2/121.0 11-deoxycortisol 347.3/97.1
11-deoxycortisol is not a good internal standard in some cases . Patients treated with Metyrapone Metyrapone is a potent inhibitor of the conversion of 11-deoxycortisol (11-DOC) to cortisol and is used in the treatment of Cushing's syndrome. . Patients with high ratio of 11-deoxycortisol to cortisol (adrenocortical carcinoma).
Work to be done: D2-cortisol as internal standard? Calibration curve? Sensitivity? Precision? Interference? Comparison with immunoassay?