Download
1 / 40

E N D
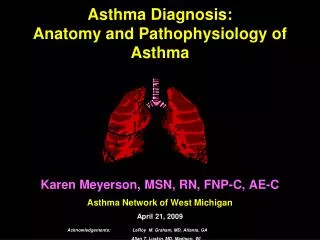
Definition of asthma “A chronic inflammatory disorder of the airways … in susceptible individuals, inflammatory symptoms are usually associated with widespread but variable airflow obstruction and an increase in airway response to a variety of stimuli. Obstruction is often reversible, either spontaneously or with treatment.” Diagnosis and natural history. Thorax 2003; 58 (Suppl I): i1-i92
Diagnosis of asthma in adults • Symptoms (episodic/variable) • wheeze • shortness of breath • chest tightness • cough Consider the diagnosis of asthma in patients with some or all of these features Diagnosis and natural history. Thorax 2003; 58 (Suppl I): i1-i92
Diagnosis of asthma in adults • Symptoms (episodic/variable) • wheeze • shortness of breath • chest tightness • cough • Signs • none (common) • wheeze – diffuse, bilateral, expiratory ( inspiratory) • tachypnea Consider the diagnosis of asthma in patients with some or all of these features Diagnosis and natural history. Thorax 2003; 58 (Suppl I): i1-i92
Diagnosis of asthma in adults • Symptoms (episodic/variable) • wheeze • shortness of breath • chest tightness • cough • Signs • none (common) • wheeze – diffuse, bilateral, expiratory ( inspiratory) • tachypnea Consider the diagnosis of asthma in patients with some or all of these features • Helpful additional information • personal/family history of asthma or atopy • history of worsening after aspirin/NSAID, blocker use • recognised triggers – pollens, dust, animals, exercise, viral infections, chemicals, irritants • pattern and severity of symptoms and exacerbations Diagnosis and natural history. Thorax 2003; 58 (Suppl I): i1-i92
Diagnosis of asthma in adults • Symptoms (episodic/variable) • wheeze • shortness of breath • chest tightness • cough • Signs • none (common) • wheeze – diffuse, bilateral, expiratory ( inspiratory) • tachypnea Consider the diagnosis of asthma in patients with some or all of these features • Helpful additional information • personal/family history of asthma or atopy • history of worsening after aspirin/NSAID, blocker use • recognised triggers – pollens, dust, animals, exercise, viral infections, chemicals, irritants • pattern and severity of symptoms and exacerbations • Objective measurements • >20% diurnal variation on 3 days ina week for 2 weeks on PEF diary • or FEV115% (and 200ml) increase after short acting ß2 agonist or steroid tablets • or FEV1 15% decrease after 6 minutes of running exercise • histamine or methacholine challenge in difficult cases Diagnosis and natural history. Thorax 2003; 58 (Suppl I): i1-i92
Indications for referral ofadults with suspected asthma • Diagnosis unclear or in doubt • Unexpected clinical findings e.g. crackles, clubbing, cyanosis, heart failure • Spirometry or PEF measurements do not fit the clinical picture • Suspected occupational asthma • Persistent shortness of breath (not episodic, or without associated wheeze) • Unilateral or fixed wheeze • Stridor • Persistent chest pain or atypical features • Weight loss • Persistent cough and/or sputum production • Non-resolving pneumonia Diagnosis and natural history. Thorax 2003; 58 (Suppl I): i1-i92
Non-pharmacologicalmanagement • Little evidence for effectiveness in preventing development of asthma, or reducing its impact • Early wheezing may be reduced with breast feeding and smoke-free environment • Allergen reduction may reduce impact of asthma • No consistent evidence supporting use of complementary or alternative treatments Non-pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
Asthma control Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
Asthma control Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
Asthma control Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
Stepwise management ofasthma in adults Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
Stepwise management of asthma in adults Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
Stepwise management of asthma in adults Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
Stepwise management ofasthma in adults Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
Stepwise management ofasthma in adults Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
Stepwise management ofasthma in adults Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
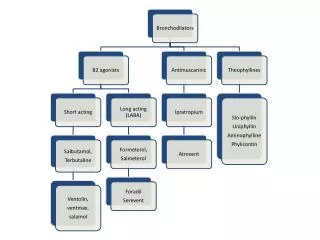
Overview: Pharmacologicalmanagement • Add inhaled long-acting 2 agonists rather than increasing the dose of inhaled steroids (above 800mcg/day in adults and 400mcg/day in children) • Step down therapy to lowest level consistent with maintained control Pharmacological management. Thorax 2003; 58 (Suppl I): i1-i92
Delivery of ß2 agonists Inhaler devices. Thorax 2003; 58 (Suppl I): i1-i92
Case discussion • BOB
Delivery of inhaled steroids Inhaler devices. Thorax 2003; 58 (Suppl I): i1-i92
Use and care of spacers Inhaler devices. Thorax 2003; 58 (Suppl I): i1-i92
Patients at risk of developingnear fatal or fatal asthma Recognised by combination of: and Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Patients at risk of developingnear fatal or fatal asthma Recognised by combination of: and Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Patients at risk of developingnear fatal or fatal asthma Recognised by combination of: and Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Lessons learnt fromstudies of asthma deaths • Many deaths from asthma are preventable – 88-92% of attacks requiring • hospitalisation develop over 6 hours • Factors include: • inadequate objective monitoring • failure to refer earlier for specialist advice • inadequate treatment with steroids Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Assessment and management of acute asthma in adults in general practice Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Assessment and management of acute asthma in adults in general practice Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Treatment of acute asthmain adults in general practice Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Hospital discharge andfollow up after acute asthma • GP review within 48 hours • Monitor symptoms and PEF • Check inhaler technique • Written asthma action plan • Modify treatment according to guidelines for chronic persistent asthma • Address factors that could have contributed to admission Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Overview: Managementof acute asthma • Assess and act promptly in acute asthma • Admit patients with any feature of a life threatening or near fatal attack, or severe attack persisting after initial treatment • Measure oxygen saturation • Use steroid tablets • Primary care follow up required promptly after acute asthma Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Patient education • Every asthma consultation provides an opportunity to review and reinforce self-management skills Patient education and self-management. Thorax 2003; 58 (Suppl I): i1-i92
Practical tips forimproving concordance • Use open questions (e.g. “If we could make one thing better for your asthma what would it be?” to understand patient’s agenda • Make it clear you are listening and responding to the patient’s concerns and goals. • Reinforce practical information and negotiated treatment plans with written instruction • Consider reminder strategies • Recall patients who miss appointments Concordance and compliance. Thorax 2003; 58 (Suppl I): i1-i92
Routine primary care Organisation and delivery of care. Outcomes and audit. Thorax 2003; 58 (Suppl I): i1-i92
Monitoring morbidity: Royal College of Physicians three questions • Applies to all patients with asthma aged 16 and over. • Only use after diagnosis has been established. Outcomes and audit. Thorax 2003; 58 (Suppl I): i1-i92
Case discussion • Susan
The British Thoracic Society Scottish Intercollegiate Guidelines Network Special asthma Occupational asthma. Thorax 2003; 58 (Suppl I): i1-i92
Occupational asthma • About 10% of adult onset asthma may be occupational • Occupational asthma is now the commonest industrial lung disease in the developed world • Patients with pre-existing asthma aggravated non-specifically by dust and fumes at work (work-aggravated asthma) should be distinguished from those with pre-existing asthma who become additionally sensitised to an occupational agent Occupational asthma. Thorax 2003; 58 (Suppl I): i1-i92
Confirming and managing occupational asthma Occupational asthma. Thorax 2003; 58 (Suppl I): i1-i92
Asthma in pregnancy • Continue treatment as usual • Monitor pregnant women with asthma closely to ensure therapy is appropriate for symptoms • Acute severe asthma in pregnancy should be treated as usual, but in a hospital setting • If anaesthesia is required, regional blockade is preferred Asthma in pregnancy. Thorax 2003; 58 (Suppl I): i1-i92